NYTimes
March 11, 2001
The Claritin Effect; Prescription for Profit
By STEPHEN S. HALL
It had been yet another miserable, nose-dripping, red-eyed spring a couple of years ago, when I finally went to see an allergy specialist. I've been battered by seasonal allergies all my life but relied on family doctors and, more recently, ''primary-care physicians'' for relief. In a kind of a pharmaceutical version of playing catch with Dad, my father and I shared his hay-fever pills when I was growing up. They were smooth, round yellow tablets, etched with a tiny red corporate symbol that was as delicate as a Chinese ideograph. At a time before people routinely gobbled down a half dozen medicines a day, those pills held a kind of mythic power for me, not only because they could make the misery of allergies disappear but also because they were prescription drugs -- inherently more powerful, more inaccessible, more special.
Those yellow pills were called Chlor-Trimeton, manufactured by the Schering-Plough Corporation, first as a prescription drug and then, after 1976, as an over-the-counter medication. It definitely worked, but it knocked me out. I remember days when I felt glazed by sleepiness. Even as the high tide in my nose and throat subsided, I felt mentally waterlogged.
For the most part, I managed to get by with over-the-counter medications until that spring in 1999, when I decided I needed something stronger. After rummaging through a cabinet in the examining room, my new allergist handed me a week's supply of Claritin, also made by Schering-Plough. Claritin was, and still is, the most frequently dispensed drug sample in the United States, part of the nearly $8 billion worth of free drug samples that pharmaceutical companies distribute to doctors annually. I had seen the ads on TV -- who hadn't? I figured I'd give it a try.
Claritin had several other distinctions: it was by then the best-selling antihistamine in the United States, indeed the most profitable antihistamine of all time, with annual sales of more than $2billion. And it was the most aggressively marketed drug to American consumers. Claritin is a drug for our time: designed to relieve symptoms and improve ''quality of life,'' hardly lifesaving or even curative, expensive as hell. A month's supply of Claritin currently costs about $80 or $85 in the United States, even though it is an over-the-counter drug in dozens of other countries, where it usually costs $10 or $15. The high domestic price is paired with an enormous potential market: an estimated 35 million Americans suffer seasonal allergies, and many of us will be feeling that first tickle of dread later this month, when spring tree pollen begins to barge into our air passages like molecular roustabouts.
So I went home and tried it. The little white pill was easy to swallow and had to be taken only once a day. There was just one problem: it didn't work. It didn't relieve my runny nose and red-rimmed, gunked-up eyes. When I told my allergist, he didn't seem particularly surprised. Only about 30 to 40 percent of his patients, he said, found the drug helpful. And, he added, that estimate was ''generous.'' I was surprised, perhaps naïvely, by this remark. I figured a ''blockbuster'' drug would be efficacious in more than 50 percent of the people who took it. The percentage he mentioned, incidentally, is certainly debatable; in fact a debate broke out later between my allergist and his partner, who thought 50 or 55 percent was more like it. Even so, it made me wonder: $80 for a drug that works only half the time?
Claritin has been singled out as a prime example of greed by the American pharmaceutical industry, notably last summer by Al Gore during his presidential campaign, and there has been a constant stream of negative press about Schering-Plough's efforts to get the basic patent on Claritin extended beyond its 2002 expiration. Schering-Plough has argued that the patent should be extended because the Food and Drug Administration review of Claritin was unusually ''protracted'' (which, in fact, it was). To press its case in Washington, the company has paid millions of dollars in political contributions and assembled a high-powered, strange-bedfellows team of lobbyists (including the former senators Howard Baker and Dennis DeConcini, the Gore confidant Peter Knight and Linda Daschle, wife of the Senate minority leader, Tom Daschle); it has also encouraged repeated attempts by Congressional supporters to insert language favorable to Schering into legislation at the last instant.
Claritin's 77-month odyssey through the F.D.A. approval process was indeed lengthy, as a General Accounting Office report, issued last August, documents. That report prompted me to read through the transcripts of old F.D.A. meetings, obtain other documents through Freedom of Information requests and speak to doctors about allergy medications in general. As I learned more about the approval of Claritin, I realized that the biography of this one drug reveals a great deal about why prescription drugs cost so much to bring to market, and also why health-care economists like Uwe E. Reinhardt of Princeton University argue that we are paying premium prices for new drugs like these without actually knowing if they are better than the drugs they've replaced. The Claritin story is an unauthorized biography, in the sense that Schering-Plough declined to grant any interviews and responded only to written questions.
It is above all a case study of how a drug company creates a blockbuster. There are no villains, no broken laws -- just an enormous expenditure of money, a highly sophisticated understanding of food and drug laws, daring marketing, a great deal of luck. Making it all possible is a financial system that ultimately passes along the high price of a modest drug to third-party payers -- and you.
Claritin's journey from lab bench to marketplace was nearly epic in the time it took, the vicissitudes encountered and the plot twists along the way. In June 1980, when Schering filed a patent for the group of chemical compounds that included the drug that would eventually be known as Claritin, the world of drug development was quite different. It typically cost a pharmaceutical company roughly $200 million to $250 million to develop a new drug; that cost is estimated to be closer to $500 million today, a figure that also accounts for failures along the way. A patent lasted 17 years from the date it was issued; it now lasts 20 years from the date the application is filed. And the effective patent life of a new drug -- the amount of time a company can expect to enjoy an exclusive run in the marketplace -- was about eight years; the average effective patent life of a drug has nearly doubled since then. The Schering patent, issued Aug. 4, 1981, stated that the compounds, including the future Claritin, were ''useful as antihistamines with little or no sedative effects.'' Pharmaceutical companies rarely disclose the cost of bringing a specific drug to market, but it's a safe bet that it took at least several hundred million dollars to deliver on the promise of those nine words.
Loratadine (pronounced ''low-RAT-a-deen'') -- the generic name for Claritin -- was one of several second-generation antihistamines that emerged from drug-company laboratories in the 1980's. They worked by essentially the same simple mechanism as the first-generation antihistamines developed immediately after World War II, like Chlor-Trimeton. When pollen bumps into certain immune-system cells just beneath the lining of the nose, eyes or respiratory passages, it provokes an immunological overreaction in susceptible people. Thus perturbed, these ''mast cells'' shudder with the molecular equivalent of uncontrollable weeping; they churn out at least 15 different inflammatory molecules, many of which contribute to the allergic reaction. One of those molecules, unleashed instantaneously, is called histamine.
When these roving histamine molecules attach to receptors on nearby nerve cells, you feel an itch or a sneeze or a scratchy, ticklish palate. When they dock onto receptors in nearby blood vessels, the vessels become porous and leaky, and fluids begin to ooze into the tissues of your nose and eyes. Antihistamine drugs work because the active ingredient is a molecule that fits like a cap onto the histamine receptor, blocking the signal that causes itchy, watery symptoms.
Everyone agrees these drugs are effective, but just how effective is very difficult to say. All the antihistamine drugs, new and old, are plagued by high placebo effects. ''It's a question of how bad a placebo effect you have,'' says Dr. Peter S. Creticos, head of the allergy and clinical immunology division at the Johns Hopkins University School of Medicine. ''The placebo effect can be anywhere from 20 to 40 percent.''
Complicating the process of determining efficacy is how the data are gathered: patients in these trials typically assess their own degree of symptom relief, which many allergists concede makes the data somewhat subjective.
Then there's the sponsorship of the science. Because the placebo effect is so high, large numbers of patients must be enlisted in clinical trials to achieve a robust, or statistically ''significant,'' result, which means that only drug companies can afford the expense. Studies sponsored by drug companies tend to show an advantage for the company's own products. Zyrtec, an antihistamine produced by Pfizer, for example, has been shown to be more potent than other drugs in its antihistamine effect -- in a study sponsored by Pfizer. Desloratadine, currently awaiting F.D.A. approval as the next generation ''super-Claritin,'' is said to relieve nasal stuffiness, unlike other antihistamines -- in a study done by Schering. And Allegra, produced by Aventis, was recently shown to be equal to Zyrtec -- in a study sponsored by Aventis. ''They're going to take that study all the way to the bank,'' one academic allergist chuckled. Which is precisely the point. Scientific studies of these drugs serve as marketing tools, providing drug-company salesmen with their best lines.
The first-generation antihistamines, now sold over the counter as Chlor-Trimeton, Benadryl, Tavist and others, are still considered pretty effective medicines. In fact, many allergists told me that they are at least equivalent in medical potency to newer drugs like Claritin and Allegra. But the first-generation molecules cross the blood-brain barrier and get into the central nervous system, causing drowsiness. The second-generation drugs have been medicinally engineered to stay out of the brain. As a result, they cause little or no sedation.
A nonsedating antihistamine was clearly a desirable drug, and Schering-Plough had been looking for one since the 1960's. In fact, the company thought it had one in a compound called azatadine. The drug is still sold as Optimine, and if you've never heard of it, that's because the compound looked deceptively nonsedating when it was tested in cats and showed its true, somnolent colors only during human testing. Next came loratadine. Following years of testing, Schering formally submitted what is known as a New Drug Application, or N.D.A., to the Food and Drug Administration on Oct. 31, 1986, seeking approval of loratadine.
Schering was not the first company to knock on the F.D.A.'s door with a nonsedating antihistamine. Seldane (terfenadine), manufactured by Marion Merrell Dow, had been approved the year before, and Hismanal (astemizole) was already under F.D.A. review. Because a similar nonsedating antihistamine was already on the market, the F.D.A. assigned Claritin its lowest priority for review -- it was considered, according to an F.D.A. classification system no longer in use, a drug that ''essentially duplicates in medical importance and therapeutic usage one or more already marketed drugs, offering little or no therapeutic gain over existing therapies.'' Technically, Claritin started out as a ''me too'' drug.
Schering-Plough doggedly pursued the approval of Claritin, spurred, no doubt, by the phenomenal success of Seldane. But it wasn't easy. Over six and a half years, Schering filed 37 major amendments to its application. The company decided to switch the formulation from capsules to tablets, and it took more than two years to show that the capsules used in clinical trials were pharmacologically identical to the tablets it intended to sell. Among the many obstacles Schering had to overcome, the first was to convince F.D.A. reviewers of the drug's main selling point: that it could be effective without causing drowsiness.
To approve a new drug, the F.D.A. must be convinced that it is both safe and effective. As a practical matter, that often means arriving at a balance between potency and side effects. Drug companies routinely submit notebooks of dictionary girth full of experimental results establishing a drug's safety profile, first in animals and then in human subjects. In establishing the effectiveness of a new drug, however, a company has only to show in well-designed trials that a drug is more effective than a sugar pill, and if there is already an equivalent drug on the market for the same use, that it is at least equally effective.
The effectiveness of loratadine had been an area of F.D.A. concern as early as January 1987, just months after Schering filed its application. Dr. Sherwin D. Straus, the F.D.A. medical officer assigned to review the drug, told the company that a 10-milligram dose of Claritin -- the amount marketed today -- did not appear to be very effective. He reiterated that point in public on Oct. 23, 1987, when the F.D.A.'s Pulmonary-Allergy Drugs Advisory Committee met at the agency headquarters in Rockville, Md., to consider Schering's application for loratadine. (This panel of outside experts doesn't formally approve new drugs, but makes influential recommendations to the agency.)
Establishing a drug's safety and efficacy is not a pretty business. A parade of Schering representatives described a staggering amount of data from animal tests in mice, rats, guinea pigs, cats and monkeys, including the ''mouse-paw edema test'' (in which mice have their paws cut off and weighed to see how successfully an antihistamine inhibits swelling). In several studies, extremely high doses of the drug, consumed daily for up to two years, produced borderline evidence of liver-tumor formation in rats and male mice, but otherwise loratadine appeared very clean. Indeed, the company maintains that the drug's ''excellent safety profile is well established'' by 10 billion ''patient days'' of experience in the marketplace.
After preclinical animal tests, Schering began to test loratadine in thousands of human patients, first to establish its safety and then to prove its effectiveness. The company ultimately submitted three so-called ''pivotal'' clinical trials to support the drug's safety and efficacy. Schering conducted what is considered the gold standard in drug testing -- randomized, double-blind trials pitting Claritin against both placebo and one of several already approved antihistamines -- and the results reveal just how vexing the placebo effect can be. In one study, for example, people taking Claritin experienced a 46 percent improvement in symptoms at the end of the trial; patients taking a placebo reported 35percent improvement. In another trial, Claritin produced 43 percent improvement versus 32 percent on placebo. As part of these same studies, physicians examined the patients and, unaware of which treatment each had received, assessed their condition; these doctors concluded that anywhere from 37 to 47 percent of patients taking the sugar pill showed a ''good or excellent response to treatment.''
When it was his turn to speak, Straus engaged in a little bureaucratic soft-shoe, complimenting the Schering team's presentations as ''a tough act to follow.'' Then he tried to demolish the heart of Schering's application. Straus didn't doubt that loratadine worked as an antihistamine, he said; he just doubted that it worked at the 10-milligram dose. In fact, at one point he claimed that ''10 milligrams is not very different than placebo clinically.'' The reason the dose was so low, he argued, is that evidence of sedation began to crop up at higher, more effective doses.
What he didn't say -- but what everyone understood -- is that using a higher, more effective dose of Claritin would affect how the drug was described on the label. The term ''nonsedating'' was considered a critical marketing point. A single adjective or phrase contained in the F.D.A.-approved label -- no more sedating than a sugar pill,'' for example -- can form the basis of claims made by company salesmen to doctors, the basis of words that throb in the bold type of advertisements, even the basis of lawsuits filed against competitors. Those seemingly eye-glazing, hairsplitting distinctions provide the foundation for multimillion-dollar marketing campaigns.
The clash over effectiveness was crystallized in one edgy exchange between Straus and Dr. Anthony Nicholson, a British neuroscientist, one of the Schering-sponsored clinical researchers, over the interpretation of a study that compared loratadine to a sedating antihistamine called tripolidine. ''We are not actually in the business of saying one drug is better than the other,'' Nicholson told Straus. ''We are in the business of saying whether a drug is acceptable in terms of its performance profile.''
''But how can you say it is acceptable in terms of its performance profile,'' Straus replied, ''without comparing it to what else is out there?''
''We compare it with placebo,'' Nicholson said.
''So you compare it to nothing.''
''Yes.''
''And it is better than nothing.''
''Yes.''
''All right,'' Straus said. ''I can't argue with that.''
The Schering representatives gave as good as they got. One suggested that Straus was guilty of statistical mischief; he had selectively looked at variables, subsets and time points, ''and this is, as I am sure everybody in this audience knows, the perfect method of proving any claim one wants.'' Dr. William Darrow, a senior vice president at Schering, acknowledged that Straus's concerns were legitimate, ''but for us the question is whether we have demonstrated consistently superiority and adequate efficacy over placebo by the 10-milligram dose. And we stand on our data there.''
In a sense, they were both right. Schering had shown, according to the requirements of the law, that a 10-milligram dose of loratadine was more effective, and no more sedating, than placebo. And Straus had argued, to the satisfaction of at least some people on the committee, that while the drug might be more effective than placebo, it was not a whole lot more effective.
Perhaps the most startling assertion made at that 1987 meeting came not from Straus, however, but from Leslie Hendeles, a pharmacology professor at the University of Florida, and it is as relevant to allergy sufferers today as it was back then. He suggested that most of the patients in Schering's Claritin studies would have been better off being treated with a different class of allergy medication altogether -- steroid nasal sprays. ''Certainly, in this kind of patient that was selected for this study,'' he said to the gathering, ''most clinicians would probably use intranasal steroids to provide very prompt and sustained relief, rather than antihistamines.'' To treat full-blown allergy symptoms with an antihistamine, he continued, was ''pharmacologically irrational.''
Hendeles and other experts made a similar point to me recently: steroid nasal sprays, like Flonase and Schering's own Nasonex, shut off an allergic reaction that's already under way. In 1998, the Annals of Allergy, Asthma and Immunology published treatment guidelines stating that these nasal sprays ''are the most effective medication class for controlling symptoms'' of allergies. The popular antihistamines are valuable at preventing an allergy attack from getting under way if taken ahead of time and seem to be effective against eye symptoms, but they rarely bring quick and substantial relief of nasal symptoms once histamine has already begun to wreak havoc. ''We don't use these medicines correctly,'' said Peter Creticos of Johns Hopkins. ''As I tell patients, by the time the process starts, the horse is already out of the barn in terms of the antihistamines. You turn the process off by using a nasal steroid.''
Although the F.D.A. advisory committee recommended approval of loratadine, Straus remained skeptical. In the conclusions of a 321-page ''medical officer review'' dated Nov. 9, 1987, he described the proposed 10-milligram dose of Claritin as ''minimally effective versus placebo'' and added that 40 milligrams appeared to be ''the minimum effective dose.'' He also argued that the label ''must include sedation as an adverse reaction and include warnings to this effect.'' A former F.D.A. official, who requested anonymity, said that the agency informally asked Schering to test a higher dose of loratadine but lacked the regulatory authority to mandate it.
By May 1988, however, the F.D.A. had come to the conclusion that the 10-milligram dose was no more sedating than a placebo pill, and by July 1989, as the General Accounting Office report puts it, ''a consensus had developed at F.D.A. that 10 milligrams was effective.'' It is impossible to determine whether Sherwin Straus had changed his mind. Around the time he was assessing loratadine, according to former colleagues, he developed multiple sclerosis and became seriously ill, eventually dying of the disease.
''Schering-Plough always believed that loratadine was safe and effective at the 10-milligram dose,'' William O'Donnell, a company spokesman, wrote in reply to a question, ''and felt that the clinical studies that were done fully supported that conclusion.''
Pharmaceutical executives rarely talk about luck as a feature in the process of drug development, but in 1989 alone, Claritin's fortunes were buffeted like a grain of pollen in an early spring breeze. In September of that year, the acting division director at the F.D.A., reviewing the drug's status, concluded that all outstanding issues regarding safety, efficacy and the equivalence of tablets and capsules had been resolved. Claritin should have been nearing approval. But earlier in the year, as part of an F.D.A. reorganization, the Claritin application was transferred to a different division within the F.D.A.; with the transfer came a new pharmacology reviewer. This reviewer revisited some toxicology issues Schering thought had been settled.
Around this time, according to Schering, tests on other products being conducted at the F.D.A.'s National Center for Toxicological Research in Jefferson, Ark., were showing that high doses of doxylamine, an antihistamine and sleep aid, produced liver tumors in rodents. These findings apparently prompted the F.D.A. to reconsider results of animal experiments with both loratadine and cetirizine (the active ingredient in Zyrtec); they, too, had shown increases in liver adenomas, abnormal growths that were then considered to be a ''larval'' form of malignant tumor.
The stakes for Claritin were high. If a prescription drug caused cancer in animals but was of medical importance, and if no satisfactory alternative existed, the usual procedure would be to approve the drug and describe the findings on the drug's label, said Paula Botstein, then a deputy F.D.A. director, at a 1991 meeting. But if similar drugs were already on the market and were not carcinogens, she said, the F.D.A. would ''ordinarily'' not approve a new drug if it caused cancer in animals. Both Seldane and Hismanal were already on the market, and neither caused cancer in animals. Because of this situation, said a former F.D.A. official who asked not to be named, the Claritin approval was ''certainly'' in doubt -- even after an advisory panel concluded that it was unlikely to pose a cancer risk to humans. (The other two drugs, doxylamine and cetirizine, were also cleared of suspicion.) Nevertheless, the F.D.A. still insisted on further tests, which eventually convinced agency officials that the drug was safe. Schering-Plough has always insisted that Claritin is not a carcinogen.
While these safety concerns were being investigated, a fateful new chapter in the Claritin story began to unfold. On a night in November 1989, in what first looked like an unrelated event, a 39-year-old woman was brought to the National Naval Medical Center in Bethesda, Md., after fainting while driving on the Washington Beltway. She had lost consciousness four times in a two-day period. She was taking the antihistamine Seldane (not for allergies but for a sinus condition) and then began using an antifungal drug, ketoconazole, to prevent a vaginal yeast infection. ''And that turned out to be a deadly combination,'' recalled Dr. Brian P. Monahan, who treated the woman for potentially fatal cardiac arrhythmias.
As doctors investigated this unusual case, they uncovered previous reports of dangerous irregularities in heartbeat among Seldane patients. Later they found that risk in Seldane patients to be associated with ketoconazole or erythromycin, a widely used antibiotic. In August 1990, at the F.D.A.'s urging, Seldane's manufacturer, Marion Merrell Dow, sent letters to doctors warning of these potentially fatal drug interactions, and in 1992 the F.D.A. ordered warning statements, outlined by a prominent black box, to appear at the top of the label and packaging on Seldane and Hismanal.
This turned out to be very good news for Claritin. Because of growing concerns about the two other nonsedating antihistamines, the F.D.A. ''started to believe that it would be beneficial to have Claritin for sale,'' according to G.A.O. investigators. (Schering said in a statement, ''We do not believe that loratadine was the result of a balancing of product-safety issues.'')
In the span of several years, therefore, Claritin had gone from being a me-too drug, to one that looked possibly unapprovable, to the only game in town. This regulatory roller coaster finally came to a rest in April 1993 when, 77 months after Schering applied, the F.D.A. approved loratadine.
At least one analyst, Mara Goldstein of C.I.B.C. World Markets, estimates that Schering-Plough lost $4billion in revenues because of the delay. But I heard
a different view from a pharmacologist who, although insisting on anonymity, was familiar with these unfolding events. ''I think they've grossly benefited from the delay at the agency,'' this researcher told me. ''Because terfenadine'' -- the generic name for Seldane -- was getting blasted, they looked like a good alternative, and I think they actually got a much larger share when they hit the market because of it.''
Since Claritin's approval, the marketing campaign for the drug has rewritten the rules for pharmaceutical promotion. The brand is ubiquitous: watching the World Series in 1999, viewers frequently saw Claritin proclaimed the ''official allergy medication of Major League Baseball''; the bag the pharmacist gives you when you fill almost any prescription suggests that you ''ask your pharmacist about Claritin-D 24 Hour.''
The direct-to-consumer ads seen on TV and in magazines are only the tip of the iceberg. The bulk of pharmaceutical marketing goes on behind closed doors, where drug salesmen tout their products to doctors, and pharmaceutical companies now spend more than $13 billion a year on such promotion, according to I.M.S. Health, a company that tracks the pharmaceutical business. The language of those presentations is constrained by the language on the F.D.A.-approved label -- in other words, all the battles over efficacy and sedation at those obscure F.D.A. meetings in the 1980's define the sales vocabulary of the 1990's.
Once again, Claritin was the beneficiary of some lucky timing. In August 1997, the F.D.A. relaxed its rules governing television advertising; rather than having to run the same fine print required in magazine ads, commercials could satisfy F.D.A. rules by giving a toll-free number, mentioning a magazine advertisement and instructing viewers to ''ask your doctor'' for more information. In a daring move closely watched by the rest of the industry, Schering-Plough poured $322 million into pitching Claritin to consumers in 1998 and 1999, far more than any other brand, according to the National Institute for Health Care Management Foundation, a nonprofit group in Washington.
''That campaign was a landmark,'' says the group's Steven D. Findlay. ''The Claritin campaign, along with Viagra, Prilosec and a few other high-profile drugs, was very influential. Claritin was clearly the most visible, the most expensive and skillfully executed, and the bottom-line results were immediately apparent. It had a huge impact, because everybody is watching everybody else very closely.'' Drug companies spent an estimated $2.5 billion on consumer advertising in 2000; these ads may have brought in as much as a $5-to-$6 return for each dollar spent.
Yet critics point out that direct-to-consumer advertising illustrates an embarrassing paradox: marketing may be most indispensable in categories where new drugs may actually be less innovative. ''Marketing is meant to sell drugs,'' Marcia Angell wrote in an editorial in The New England Journal of Medicine last June, ''and the less important the drug, the more marketing it takes to sell it. Important new drugs do not need much promotion. Me-too drugs do.''
But promotion works. Sales in the United States of the entire Claritin family -- not just the 10-milligram tablets, but a syrup, quick-dissolving RediTabs and both 12-hour and 24-hour Claritin-D versions with a decongestant -- which stood at $1.4 billion in 1997, jumped to $2.6 billion by 2000. It accounts for nearly 30 percent of Schering-Plough's annual revenues.
Schering had a magnificent cash cow. Now the trick was to milk it as long as possible.
Almost from the moment Claritin was approved in 1993, with only five years remaining on its basic patent at the time, Schering-Plough and its competitors began to tussle over the drug's afterlife -- and, more important, when it would begin. Generic drug companies typically gear up to produce a cheap version of a drug about five to seven years before a patent is due to expire. Schering, at that same time, began to mount its expensive legislative campaign to extend Claritin's patent. This fundamental conflict, played out in Congress and in court, is shaping the golden years of Claritin's already eventful career as a drug.
The Claritin patent has been extended several times already, each extension reflecting laws passed by Congress in the last two decades that have modernized the F.D.A. review process and significantly extended the effective life of drug patents. The extensions began with the Drug Price Competition and Patent Term Restoration Act of 1984, known informally as the Hatch-Waxman Act. Despite its dense legal provisions, Hatch-Waxman is an essential element of any conversation about drug prices in this country. The law was a legislative high-wire act designed to reward innovation at major pharmaceutical companies and protect intellectual property while at the same time promoting lower drug costs, primarily by making it easier for generic drug makers to get to the American marketplace. As part of Hatch-Waxman, new drugs being developed after the law was enacted in 1984 could receive automatic patent extensions of five years. More than 100 drugs, including Claritin, were already in development when the law was passed; these products, known as ''pipeline'' drugs, were eligible for only two years. That reset the clock for Claritin's patent expiration to the summer of 2000.
In 1994, the Uruguay Round Agreements Act, an obscure addendum to the GATT treaty, added 22 months to the patent life of Claritin, pushing the expiration back to June 2002. And just last August, the basic patent on Claritin was extended yet another six months, to December 2002, because Schering-Plough conducted pediatric trials of the drug. If six months doesn't sound like a lot, consider the economic incentive here: for the price of a modest clinical trial in children (costing at most $3 million), Schering can extend the life of its basic patent half a year and earn close to $1billion. By one unofficial estimate, these three patent extensions will ultimately translate into additional Claritin revenues totaling about $13 billion.
Since 1996, there have been at least a half dozen attempts to extend Claritin's patent life even more. There was an attempt, for instance, in the summer of 2000 to slip language at the last minute into a military-appropriations bill. Schering's lobbying efforts have not been the most persistent, ''just the crudest,'' according to Bruce Downey, C.E.O. of Barr Laboratories, a generic drug maker based in Pomona, N.Y., who has also testified against extending the Claritin patent.
Representative Waxman has derided the legislation proposed to provide Schering relief as the ''Claritin Monopoly Relief Act.'' But the case for some of the pipeline drugs may not be as outrageous as some critics have suggested. Peter Barton Hutt, the former chief counsel at the F.D.A. and now a lawyer at the Washington firm Covington & Burling, has argued that limiting loratadine and several other pipeline drugs to a two-year extension was ''completely arbitrary'' and assumed much speedier approval.
As has been true of so much of this drug's history, however, timing is everything, and Schering-Plough's efforts to extend its monopoly has coincided with surging public discontent about the cost of drugs. As a result, each attempt by the company to get Congressional patent relief has become a rallying cry for opponents, including consumer watchdogs, health insurers and generic drug makers. Since the 1996 election, Schering has spent $19.9 million on lobbying and campaign contributions, according to the watchdog group Public Citizen. Yet the most tangible achievement to date of that $20 million lobbying campaign may be the way that it has galvanized the generic drug industry and attracted the attention of lawmakers. Last fall, Senators John McCain and Charles Schumer introduced legislation designed to close loopholes in Hatch-Waxman.
For all the closed-door maneuvering in Washington, an equally revealing pharmaceutical endgame has been playing out, slowly, in a courtroom in New Jersey.
A chilly day in January, about two dozen dark-suited patent attorneys gathered in the United States District Court in Newark, in what has become a typical chain of events toward the end of a prescription drug's life: patent litigation. Unlike the arguments made by Schering-Plough's lobbyists in Washington, however, those made by its lawyers in court documents maintain that Claritin's patent protection extends beyond 2002.
Last August, Teva Pharmaceuticals became the first company to receive tentative approval from the F.D.A. to market a generic version of Claritin. The key word here is ''tentative.'' Teva must wait for the basic loratadine patent to expire next year. It must wait for the resolution of a lawsuit filed against it by Schering, which could conceivably stretch into 2003. And it must wait for Geneva Pharmaceuticals, a generic company based in Broomfield, Colo., to bring its version of Claritin to market; Geneva is entitled to an exclusive 180-day run as the only generic in the market, a monopoly that the company receives as Hatch-Waxman's reward for being the first generic drug maker to challenge a brand drug's patent. The moment the first generic enters the market, industry experts estimate, the cost of generic Claritin will drop to about 80 percent of current prices. When everyone else jumps in six months later, the price will fall off a cliff. ''With so many competitors,'' one generic executive told me, ''the price will drop to $10 very quickly.''
Generic companies fill about 42 percent of all drug prescriptions in this country, but the price disparity with brand-name drugs is striking. That market share accounted for slightly less than $20 billion in drug sales in 1999; brand company sales accounted for more than $90 billion. Industry advocates claim that if generic sales inched up to 52 percent, American consumers would save an estimated $11 billion a year in drug costs. If the generic industry is beginning to mature, as some maintain, one of the main factors in that process has been, oddly, Schering-Plough. ''I think loratadine is one of the first examples,'' said Dr. Carole Ben-Maimon, head of the Generic Pharmaceutical Industry Association and until recently a vice president at Teva. ''We were really able to make it an issue.''
Much of the industry's current disgruntlement involves patent litigation -- or as George S. Barrett, president and C.E.O. of Teva USA puts it, ''the way the patent system has just been abused.'' When Congress devised the language of Hatch-Waxman back in 1984, the notion of a drug coming ''off patent'' was as simple as it sounds: once the patent for a basic compound expired, other companies were free to enter the market. But it's not that simple anymore, said Ben-Maimon, a physician who now heads a research division at Barr.
Brand companies now patent the process of manufacturing the raw material. They patent the medical uses to which the drug can be applied. They patent the formulation of the medicine (the other ingredients used to stabilize the drug). They can patent what's known in the industry as ''trade dress'' -- the color, size and shape of the pill. They patent metabolites -- the chemicals into which a drug breaks after being metabolized by the human body.
So drugs don't come ''off patent'' the way the 1984 law envisioned; they come off as a series of strategically staggered patents, a practice known as layering. And here's where Hatch-Waxman has inadvertently turned into a playbook for complicated, time-consuming -and, according to generic drug makers, frivolous -- patent litigation.
On Feb. 5, 1998, Geneva Pharmaceuticals filed what's known as an abbreviated new drug application, or ANDA, seeking F.D.A. permission to sell a generic version of Claritin. Several days later, as obliged by Hatch-Waxman, Geneva notified the patent holder, Schering, of its plans. On March 19, Schering-Plough sued Geneva and its parent corporation, Novartis, claiming that two of its Claritin patents had been infringed. Since then, seven other drug makers -- Zenith Goldline, Teva Pharmaceuticals, Mylan, Andrx, Impax, American Home Products and Apotex-Novex -- have gone to the F.D.A. seeking approval to sell generic versions of Claritin. Although the issues vary from case to case, Schering has sued all of them.
Some critics make the case that since Hatch-Waxman, an inordinate amount of innovation has been displaced from research to litigation strategies. A lawsuit is far cheaper (about $5million per case) and less risky than research, and the return on investment can be very high. ''It's always cheaper to litigate than to lose market share,'' said a former top-level F.D.A. official who asked not to be named. ''If you can keep a generic off the market for one day, three days, five days, two months or two years, that's a lot of revenue. Certainly a lot more than it would cost to pay your lawyers.'' A Schering spokesman says, ''Schering-Plough believes that its patents are valid and enforceable.''
William Fletcher, president of Teva North America, knows how frustrating this can be. ''You know, people here have asked us several times, 'Why bother doing Claritin?''' he said. ''There are going to be at least 10 competitors out there. The price is going to be, you know, 5 percent of Claritin. Why bother doing it? One reason is that we are a broad-line supplier, and we have to have every product in our line. The other reason is that we're just bloody-minded about it, quite frankly. Stubborn. You know, you're damned if you're going to let Schering-Plough get away with it!''
There's a larger game in play in the Newark courtroom, too, according to the generic companies, and it became more interesting a few weeks ago. As Schering-Plough holds the generics at bay with one hand, it had hoped to receive F.D.A. approval in time to introduce desloratadine, its second-generation version of Claritin that will be marketed as Clarinex, this spring. ''The longer the litigation is dragged out,'' says Elliot F. Hahn, president of Andrx, ''the more opportunity they have to market desloratadine to physicians and switch them from the Claritin line to the desloratadine line.'' But that plan ran into a major snag in mid-February, when Schering-Plough revealed that the approval of desloratadine was being held up until the company corrects manufacturing deficiencies cited by the F.D.A. at four of its plants.
What to do in a crisis? Market! Several days later, as the company's stock plunged and attorneys hustled to organize shareholder lawsuits, Schering-Plough announced big new ''consumer education'' and pharmacy programs for Claritin -- the ''largest and most comprehensive allergy initiative of its kind.'' The company plans to distribute 35 million free drug samples to doctors, 6 million allergy brochures, 65,000 drugstore displays and, yes, 350 million more of those little blue pharmacy bags.
Finally, an edifying case of sticker shock. Late last fall, my allergist prescribed a month's supply of Claritin-D to clear up some congestion before I started my first round of allergy desensitization shots. The pharmacy had misplaced my insurance number, so when I went to pick up the prescription, the clerk handed me a bill for $103. This is the consumer's trickle-down tab for the roughly $250 million in drug development, more than $100 million a year in consumer advertising, many millions in closed-door marketing, $20 million in lobbying and political contributions, $5 million a year for litigation. I was stunned that it was so expensive, and I asked myself a question that is a normal part of every marketplace but health care. If I had to pay $103 out of my own pocket, would I buy this medicine? Was it worth it?
With the exception of elderly people on Medicare and the uninsured, most of us never ask that question. In a recent conversation, Gillian Shepherd, a Manhattan allergy specialist, addressed the same point, noting that antihistamines like Claritin and Allegra are about equal in potency to over-the-counter drugs like Chlor-Trimeton. And while some patients experience sedation with these drugs, many do not. ''Fifty percent of the population can tolerate most of them without any sedation,'' she explained. ''The feeling is that if there's a chance of sedation and third parties are paying, why not use the nonsedating drugs? If people were paying out of pocket, the story would be completely different.''
As I labored to sort through all the clinical data and all the confusing advertising, I found myself wishing that we had reviewers who would talk bluntly about new drugs, who could discuss efficacy, safety and value from the consumer's point of view, who could deconstruct the advertising, who would include cost as a criterion. But those are medical judgments, some would say, and only doctors should dispense them. True, but many doctors, it turns out, have largely abdicated that responsibility -- they rarely know what a drug costs, and as Shepherd mentioned, many learn about the properties of a given drug not from the medical literature but from company salesmen, who are paid to tell one-sided stories.
And so what? Richard Kogan, Schering's C.E.O., testified before Congress two years ago that drug companies need constant and ample revenue streams to support their enormous and dicey R&D enterprise, and he's right. In order to be competitive in this post-genomic era, large pharmaceutical companies need to spend $2 billion to $4 billion a year on research to develop new drugs. The industry has developed many remarkable medicines, and more are on the way.
But if high drug prices are a kind of innovation tax for American consumers, we should at least demand innovation in return. Many high-priced, successful drugs, like Zyrtec, are developed overseas and simply marketed here by American companies. Moreover, a significant amount of pharmaceutical innovation currently occurs in the biotech sector, where small, cutting-edge companies typically license their discoveries to big pharma, which has the marketing expertise. What innovative new drugs does Schering, for example, have in the pipeline, subsidized by the billions of dollars earned from Claritin? Financial analysts are mixed on the company's potential treatments -- for cancer, asthma, high cholesterol and several other major diseases -- but a leading candidate for future blockbuster status is . . . desloratadine, the chemical that is the principal metabolite, or breakdown product, of Claritin. Anyone who has taken Claritin has already had desloratadine in his or her body.
No one has seen much clinical data on the new drug, but many pharmacologists told me that metabolites rarely possess significantly more potency than their parent compounds, and one allergist confided, not for attribution: ''The only reason I can see scientifically for bringing this out is that their patent is about to expire. There have been about 20 abstracts published for desloratadine, all from Schering and all saying there's a little edge here, a little edge there, none of which strike me as terribly important.'' But then, as the Claritin story makes clear, it's not always about innovation but rather about finding little edges here and there and then marketing the hell out of them.
Meanwhile, the laboratory of Raymond Woosley of Georgetown University has done research on an over-the-counter antihistamine, Schering's own Chlor-Trimeton -- the same one my father shared with me decades ago. The lab has shown through sophisticated molecular-binding experiments that Chlor-Trimeton is more potent at grabbing and hanging onto the histamine receptor than any other antihistamine it has tested. For several years, the lab has wanted to test a lower -- and possibly nonsedating -- dose of the drug, to no avail. ''We did a grant for four years for the N.I.H., and we didn't get it funded,'' Woosley said. ''We assumed the innovator company didn't want to do it because they were making Claritin, and the generic companies didn't want to do it because it would cut into their profit margins even more.''
Woosley's study might work; it might not. The issue is that our health-care system has evolved to the point where there is no economic incentive even to try. For an industry that prides itself on taking risk, the risk of discovering that cheaper, older medicines might be just as good, and perhaps even better, than expensive new versions is apparently one risk too great to take.
Stephen S. Hall is a contributing writer for the magazine. He is working on a book about the molecular biology of aging.
Tuesday, May 30, 2006
Saturday, May 13, 2006
Quick clinics in stores
NYTimes
May 14, 2006
Attention Shoppers: Low Prices on Shots in the Clinic Off Aisle 7
By MILT FREUDENHEIM
Everyday low prices on strep-throat exams.
That is the basic idea behind a retail approach to routine medical care now catching on among consumers and entrepreneurs. At Wal-Mart, CVS and other chain stores, walk-in health clinics are springing up as an antidote to the expense and inconvenience of full-service doctors' offices or the high-cost and impersonal last resort of emergency rooms.
For a $30 flu shot, a $45 treatment for an ear infection or other routine services from a posted price list, patients can visit nurse practitioners in independently operated clinics set up within the stores — whose own pharmacies can fill prescriptions.
"It was a lot easier to know you can just drive up the block to a clinic, rather than spend time in the pediatrician's waiting room," said Liz Lyons, who recently took her 9-year-old son to have a sore throat swabbed in a clinic at a CVS drugstore in Bethesda, Md.
She made a $10 co-payment, with her husband's insurance picking up the rest of the $59 tab.
About 100 of these clinics, which typically lease space from the host stores, are now operating around the nation. Hundreds more are in the works, bankrolled by a range of competing entrepreneurs who include Stephen M. Case, the former AOL chairman; Richard L. Scott, who once ran the nation's largest hospital chain; and Michael Howe, a former chief executive of the Arby's restaurants group.
Despite their diverse backgrounds, those executives and others share a concept of "consumer-directed health care" — a marketing and political term that usually means higher out-of-pocket medical costs — as a mass-market opportunity. Even some family physicians say the clinics may have their place in the array of American medical offerings.
And most insurers so far are welcoming retail clinics as a way to save money. The uninsured, meanwhile, typically find the clinics more affordable than most alternatives — including the for-profit storefront clinics that have long offered a full range of physician-provided medical services to a walk-in clientele.
Uwe E. Reinhardt, a professor of economics and public affairs at Princeton University, said that the store chains, with their reputations on the line, would insist that the clinics maintain high standards and low error rates. "Primary care is a neglected field in the United States, lagging other economically advanced countries," he said. "The clinics can teach the rest of our health system how primary care could be done and brought to the public. That is very important." Whether a fad or the beginning of a fundamental shift, the retail clinic trend comes in response to an erosion in employer-sponsored insurance benefits that is forcing people to pay more or all of their own health costs. It is also a reaction to the growing perception that conventional medical service for routine and preventive care has become too costly and inefficient.
" Starbucks has 10,000 locations; health care is certainly more important," said Mr. Case, who made his name and fortune on the Internet but is now betting that his chain of RediClinics at Wal-Mart, Walgreens and other retailers can be the next big thing.
Mr. Case says his epiphany came a few years ago when he took his young daughter to an emergency room on a Sunday for an ear infection. "We waited four hours and they just weren't able to see us," he recalled. "This is crazy: a society in which everything is convenient other than what people care most about, which is taking care of their health."
Mr. Case's company, Revolution Health Group, has 11 RediClinics now running, including one at a Duane Reade pharmacy on West 50th Street in Manhattan. He plans to open 90 others in various retail chains by the end of this year, and 500 within three years.
Other executives bringing their names and money to the field include Hal Rosenbluth, who sold a highly automated travel business to American Express and is now behind a clinic chain called Take Care Health Systems. It has clinics in 16 stores, and Mr. Rosenbluth has raised $77 million with an eye toward expanding to 1,400 in the next few years.
Another in the game is Dr. Glen D. Nelson, a Minneapolis surgeon and investor whose health care résumé includes 11 years as president of the Park Nicollet Medical Center in Minneapolis, head of a managed health care company and later vice chairman of the medical device maker Medtronic.
"The clinic concept is a microcosm of what you could do to the whole system to improve it and make it more consumer friendly and economical," said Dr. Nelson, the chairman of MinuteClinic, which has branches in 73 stores.
The licensed nurse practitioners who run most of the clinics typically have advanced training and referral arrangements with local doctors for cases beyond the clinics' scope. Patients with major illnesses or in need of emergency care or follow-up for a chronic condition are typically referred to doctors, hospitals and urgent care centers. Infants and toddlers will usually be sent to pediatricians or family physicians.
When Ms. Lyons recently brought her son, Daniel, to the MinuteClinic at the CVS in Bethesda, the nurse practitioner on duty was Trish Hughes, who performed a quick swab test to check for a streptococcal bacterial infection. In less than three minutes, that preliminary test came up negative; the swab was retained for further testing.
Ms. Lyons said she was pleased with the clinic experience. "I will be back," she said.
For Beth Brauning, 54, a self-employed house cleaner who is uninsured, the prices at a clinic in a CVS near Columbus, Ohio, were a big attraction. The nurse practitioner took her blood pressure and wrote two allergy prescriptions she needed.
The bill was $49 — "probably half what my doctor would have charged me," Ms. Brauning said. "It was such a good experience for me. You go to an emergency room, it's $300 to walk in the door."
Having someone in the store writing prescriptions could be a boon for pharmacy chains. "Pharmacy is 70 percent of our business," said Jim Maritan, a CVS vice president for strategy and business development. "It is a great experience having a nurse practitioner clinic on site."
But some doctors say the clinic-pharmacy relationship could create conflicts of interest. "We want to make sure that the patient is protected," said Dr. Joseph P. Annis, an anesthesiologist in Austin, Tex., who is the chairman of an American Medical Association council that studied the clinics for an A.M.A. report due out later this month.
Dr. Anne B. Francis, a pediatrician in Rochester added that it was important for children to have a physician who gets to know the family and keeps a complete health record that can help point to underlying causes of some ailments. "All ear aches are not ear infections," she said.
Although some physicians are fearful of losing business to the clinics, others say that the clinics may fill a need. Larry S. Fields, a family doctor in Ashland, Ky., who is president of the American Academy of Family Physicians, said that if the clinics "stick to this limited scope, they may have a small role in providing acute health care to people who are mildly ill, when their only other alternative at the time might be an emergency room."
The academy has issued a list of "desired attributes of retail health clinics," which the big clinic operators say they have embraced, including provision of a well-defined and limited scope of services; a formal connection with local physicians to provide "continuity of care" and supervise the nurse practitioners; and electronic health records that can be transmitted to a doctor's office.
With no need for expensive medical equipment or office space, the clinics tend to be cheap to operate — particularly since the nurse practitioners are paid $30 to $45 an hour, compared with the $65 or much more an hour that a primary care doctor can command. A store clinic can be profitable with 25 patients over a 12-hour day, clinic executives said.
Employers and insurers also see opportunities for savings. The power-tool maker Black & Decker, a self-insured employer, has subtracted $10 from its usual $25 co-payments when employees patronize MinuteClinics around Baltimore, rather than visit a doctor.
"We have had an overwhelmingly positive response from our employees," said Raymond Brusca, the vice president of benefits at Black & Decker, adding, "my medical plan comes way out ahead financially."
A clinic company with somewhat grander ambitions is Solantic. Its clinics are staffed by doctors and provide a wider range of services that include X-rays at $90 apiece (or two for $150).
For routine services, Solantic's prices may be slightly higher than at other clinics — $55 or more for a Solantic doctor visit compared with $45 to be seen by a nurse practitioner at a rival's clinic. But having doctors on staff "dramatically increases the number of services we can provide to a patient," said Richard L. Scott, the chairman of Solantic, which is based in Jacksonville, Fla.
Mr. Scott built Columbia- HCA Healthcare into the nation's largest hospital chain before being forced out in a 1997 boardroom coup fueled by government allegations of Medicare fraud. Three top officers of the company were indicted, although Mr. Scott was not cited in the case. In a separate tax dispute over deductions for executive pay, the company agreed to pay a $71 million settlement to the Internal Revenue Service."I always wanted to create a clinic business when I was in the hospital business," Mr. Scott said.
Glenn Habern, Wal-Mart's senior vice president for business development, said that Solantic and three of its rivals — RediClinics, MedPoint Express and Quick Quality Care — would be among the clinic companies leasing space in about 60 of Wal-Mart's 1,300 "superstores" by the end of this year.
"It's still a test for us," Mr. Habern said. "If customers like it we may open more. So far, we've not seen any reason not to do so." But a big Wal-Mart competitor, Target, has evidently seen drawbacks.
At the end of this month Target plans to close the 11 MinuteClinics in stores in Maryland and Minnesota; the company would not explain why. "Target will begin remodeling to open new health clinics in these stores in fall 2006," the company said in an e-mail message, without specifying who would manage the new clinics.
Dr. Nelson, at MinuteClinic, said in an interview before the breakup with Target was disclosed that "the pharmacy business is a small percentage of the Target footprint."
"Target also is very disciplined," he added. "They like to have things totally designed and controlled to their own specifications. They struggled with whether they want somebody else talking to their clients."
May 14, 2006
Attention Shoppers: Low Prices on Shots in the Clinic Off Aisle 7
By MILT FREUDENHEIM
Everyday low prices on strep-throat exams.
That is the basic idea behind a retail approach to routine medical care now catching on among consumers and entrepreneurs. At Wal-Mart, CVS and other chain stores, walk-in health clinics are springing up as an antidote to the expense and inconvenience of full-service doctors' offices or the high-cost and impersonal last resort of emergency rooms.
For a $30 flu shot, a $45 treatment for an ear infection or other routine services from a posted price list, patients can visit nurse practitioners in independently operated clinics set up within the stores — whose own pharmacies can fill prescriptions.
"It was a lot easier to know you can just drive up the block to a clinic, rather than spend time in the pediatrician's waiting room," said Liz Lyons, who recently took her 9-year-old son to have a sore throat swabbed in a clinic at a CVS drugstore in Bethesda, Md.
She made a $10 co-payment, with her husband's insurance picking up the rest of the $59 tab.
About 100 of these clinics, which typically lease space from the host stores, are now operating around the nation. Hundreds more are in the works, bankrolled by a range of competing entrepreneurs who include Stephen M. Case, the former AOL chairman; Richard L. Scott, who once ran the nation's largest hospital chain; and Michael Howe, a former chief executive of the Arby's restaurants group.
Despite their diverse backgrounds, those executives and others share a concept of "consumer-directed health care" — a marketing and political term that usually means higher out-of-pocket medical costs — as a mass-market opportunity. Even some family physicians say the clinics may have their place in the array of American medical offerings.
And most insurers so far are welcoming retail clinics as a way to save money. The uninsured, meanwhile, typically find the clinics more affordable than most alternatives — including the for-profit storefront clinics that have long offered a full range of physician-provided medical services to a walk-in clientele.
Uwe E. Reinhardt, a professor of economics and public affairs at Princeton University, said that the store chains, with their reputations on the line, would insist that the clinics maintain high standards and low error rates. "Primary care is a neglected field in the United States, lagging other economically advanced countries," he said. "The clinics can teach the rest of our health system how primary care could be done and brought to the public. That is very important." Whether a fad or the beginning of a fundamental shift, the retail clinic trend comes in response to an erosion in employer-sponsored insurance benefits that is forcing people to pay more or all of their own health costs. It is also a reaction to the growing perception that conventional medical service for routine and preventive care has become too costly and inefficient.
" Starbucks has 10,000 locations; health care is certainly more important," said Mr. Case, who made his name and fortune on the Internet but is now betting that his chain of RediClinics at Wal-Mart, Walgreens and other retailers can be the next big thing.
Mr. Case says his epiphany came a few years ago when he took his young daughter to an emergency room on a Sunday for an ear infection. "We waited four hours and they just weren't able to see us," he recalled. "This is crazy: a society in which everything is convenient other than what people care most about, which is taking care of their health."
Mr. Case's company, Revolution Health Group, has 11 RediClinics now running, including one at a Duane Reade pharmacy on West 50th Street in Manhattan. He plans to open 90 others in various retail chains by the end of this year, and 500 within three years.
Other executives bringing their names and money to the field include Hal Rosenbluth, who sold a highly automated travel business to American Express and is now behind a clinic chain called Take Care Health Systems. It has clinics in 16 stores, and Mr. Rosenbluth has raised $77 million with an eye toward expanding to 1,400 in the next few years.
Another in the game is Dr. Glen D. Nelson, a Minneapolis surgeon and investor whose health care résumé includes 11 years as president of the Park Nicollet Medical Center in Minneapolis, head of a managed health care company and later vice chairman of the medical device maker Medtronic.
"The clinic concept is a microcosm of what you could do to the whole system to improve it and make it more consumer friendly and economical," said Dr. Nelson, the chairman of MinuteClinic, which has branches in 73 stores.
The licensed nurse practitioners who run most of the clinics typically have advanced training and referral arrangements with local doctors for cases beyond the clinics' scope. Patients with major illnesses or in need of emergency care or follow-up for a chronic condition are typically referred to doctors, hospitals and urgent care centers. Infants and toddlers will usually be sent to pediatricians or family physicians.
When Ms. Lyons recently brought her son, Daniel, to the MinuteClinic at the CVS in Bethesda, the nurse practitioner on duty was Trish Hughes, who performed a quick swab test to check for a streptococcal bacterial infection. In less than three minutes, that preliminary test came up negative; the swab was retained for further testing.
Ms. Lyons said she was pleased with the clinic experience. "I will be back," she said.
For Beth Brauning, 54, a self-employed house cleaner who is uninsured, the prices at a clinic in a CVS near Columbus, Ohio, were a big attraction. The nurse practitioner took her blood pressure and wrote two allergy prescriptions she needed.
The bill was $49 — "probably half what my doctor would have charged me," Ms. Brauning said. "It was such a good experience for me. You go to an emergency room, it's $300 to walk in the door."
Having someone in the store writing prescriptions could be a boon for pharmacy chains. "Pharmacy is 70 percent of our business," said Jim Maritan, a CVS vice president for strategy and business development. "It is a great experience having a nurse practitioner clinic on site."
But some doctors say the clinic-pharmacy relationship could create conflicts of interest. "We want to make sure that the patient is protected," said Dr. Joseph P. Annis, an anesthesiologist in Austin, Tex., who is the chairman of an American Medical Association council that studied the clinics for an A.M.A. report due out later this month.
Dr. Anne B. Francis, a pediatrician in Rochester added that it was important for children to have a physician who gets to know the family and keeps a complete health record that can help point to underlying causes of some ailments. "All ear aches are not ear infections," she said.
Although some physicians are fearful of losing business to the clinics, others say that the clinics may fill a need. Larry S. Fields, a family doctor in Ashland, Ky., who is president of the American Academy of Family Physicians, said that if the clinics "stick to this limited scope, they may have a small role in providing acute health care to people who are mildly ill, when their only other alternative at the time might be an emergency room."
The academy has issued a list of "desired attributes of retail health clinics," which the big clinic operators say they have embraced, including provision of a well-defined and limited scope of services; a formal connection with local physicians to provide "continuity of care" and supervise the nurse practitioners; and electronic health records that can be transmitted to a doctor's office.
With no need for expensive medical equipment or office space, the clinics tend to be cheap to operate — particularly since the nurse practitioners are paid $30 to $45 an hour, compared with the $65 or much more an hour that a primary care doctor can command. A store clinic can be profitable with 25 patients over a 12-hour day, clinic executives said.
Employers and insurers also see opportunities for savings. The power-tool maker Black & Decker, a self-insured employer, has subtracted $10 from its usual $25 co-payments when employees patronize MinuteClinics around Baltimore, rather than visit a doctor.
"We have had an overwhelmingly positive response from our employees," said Raymond Brusca, the vice president of benefits at Black & Decker, adding, "my medical plan comes way out ahead financially."
A clinic company with somewhat grander ambitions is Solantic. Its clinics are staffed by doctors and provide a wider range of services that include X-rays at $90 apiece (or two for $150).
For routine services, Solantic's prices may be slightly higher than at other clinics — $55 or more for a Solantic doctor visit compared with $45 to be seen by a nurse practitioner at a rival's clinic. But having doctors on staff "dramatically increases the number of services we can provide to a patient," said Richard L. Scott, the chairman of Solantic, which is based in Jacksonville, Fla.
Mr. Scott built Columbia- HCA Healthcare into the nation's largest hospital chain before being forced out in a 1997 boardroom coup fueled by government allegations of Medicare fraud. Three top officers of the company were indicted, although Mr. Scott was not cited in the case. In a separate tax dispute over deductions for executive pay, the company agreed to pay a $71 million settlement to the Internal Revenue Service."I always wanted to create a clinic business when I was in the hospital business," Mr. Scott said.
Glenn Habern, Wal-Mart's senior vice president for business development, said that Solantic and three of its rivals — RediClinics, MedPoint Express and Quick Quality Care — would be among the clinic companies leasing space in about 60 of Wal-Mart's 1,300 "superstores" by the end of this year.
"It's still a test for us," Mr. Habern said. "If customers like it we may open more. So far, we've not seen any reason not to do so." But a big Wal-Mart competitor, Target, has evidently seen drawbacks.
At the end of this month Target plans to close the 11 MinuteClinics in stores in Maryland and Minnesota; the company would not explain why. "Target will begin remodeling to open new health clinics in these stores in fall 2006," the company said in an e-mail message, without specifying who would manage the new clinics.
Dr. Nelson, at MinuteClinic, said in an interview before the breakup with Target was disclosed that "the pharmacy business is a small percentage of the Target footprint."
"Target also is very disciplined," he added. "They like to have things totally designed and controlled to their own specifications. They struggled with whether they want somebody else talking to their clients."
Tuesday, May 09, 2006
Men's facial traits
May 9, 2006
Women Get Paternal Clues in Men's Faces
By THE ASSOCIATED PRESS
Filed at 9:48 p.m. ET
CHICAGO (AP) -- Women looking for a long-term relationship like men who like children -- and they can tell which guys might be interested in becoming fathers just by looking at their faces. Those are among the findings of a study of college students published Wednesday in a British scientific journal.
''This study suggests that women are picking up on facial cues that are perhaps related to paternal qualities,'' said James Roney, a University of California at Santa Barbara psychologist and lead author of the study. ''The more they perceived the men as liking kids, the more likely they could see having a longer-term relationship.''
Experts said evolution has apparently programmed women to recognize men who might be interested in propagating the species by raising a family.
The study wasn't all bad news for men not interested in settling down. It found that women can look at men's faces and figure out which of them have the highest testosterone levels. Those men -- rated the most masculine by the women -- turn out to be just the kind of guys they would want for a fling.
''Women make very good use of any information they get from a man's face,'' said co-author Dario Maestripieri, an associate professor of comparative human development at the University of Chicago. ''Depending on what they want and where they are in their lives, they use this information differently.''
In the study, published in Proceedings of the Royal Society B: Biological Sciences, researchers looked at a group of 39 men, ages 18 to 33, at the University of Chicago. Each man was shown 10 pairs of photographs and silhouettes, one of an adult and the other of an infant, and asked to rate their preferences. Meanwhile, their saliva was tested to determine testosterone levels.
Photographs of the men's faces were then shown to 29 women, ages 18 to 20, at the University of California at Santa Barbara.
The women were asked to rate the men on four qualities: ''likes children,'' ''masculine,'' ''physically attractive'' and ''kind.'' Then they were asked to rate how attractive they found each man for short-term and long-term romance.
The study found women did well at rating men on their interest in babies, and those they rated masculine generally had higher testosterone levels than the others.
For example, the men who indicated they liked children the most were rated as above average in liking children by 20 of the 29 women. The men who showed no interest in children were correctly rated as below average in that category by 19 of the women.
The higher the women rated the men for masculinity, the higher they were rated as potential short-term romantic partners. The higher they rated men for their interest in children, the higher they were rated for long-term romance.
The features that research has suggested denote high testosterone levels include a prominent jaw and a heavy beard.
The findings came as no surprise to those in the business of studying human behavior -- and love.
''What this study illustrates is that there are genetic programs that increase survival of the species because there are hormones in women that are cuing their reactions to the hormones of the men,'' said Dr. Daniel Alkon, scientific director of the Blanchette Rockefeller Neurosciences Institute in Morgantown, W.Va., and Washington.
Or as Kristin Kelly, a spokeswoman for the online dating service Match.com, put it: ''They call it `love at first sight' for a reason. They don't say `love at first sentence,' `love at first word.'''
It is unclear just what about the men's faces tipped the women off about their interest in children. While Maestripieri guessed it might have something to do with ''a more rounded face, a gentler face,'' Roney said the answer might be found in the expressions on the men's faces.
He explained that after the study was completed, five graduate students were asked to rate on a scale of 1 to 7 whether the men looked angry or happy. Though the men were instructed to have a neutral look on their faces when photographed, some apparently looked happier than others.
''It seemed that the men who picked more infants in that test had a happier or more content look on their face,'' he said.
Women Get Paternal Clues in Men's Faces
By THE ASSOCIATED PRESS
Filed at 9:48 p.m. ET
CHICAGO (AP) -- Women looking for a long-term relationship like men who like children -- and they can tell which guys might be interested in becoming fathers just by looking at their faces. Those are among the findings of a study of college students published Wednesday in a British scientific journal.
''This study suggests that women are picking up on facial cues that are perhaps related to paternal qualities,'' said James Roney, a University of California at Santa Barbara psychologist and lead author of the study. ''The more they perceived the men as liking kids, the more likely they could see having a longer-term relationship.''
Experts said evolution has apparently programmed women to recognize men who might be interested in propagating the species by raising a family.
The study wasn't all bad news for men not interested in settling down. It found that women can look at men's faces and figure out which of them have the highest testosterone levels. Those men -- rated the most masculine by the women -- turn out to be just the kind of guys they would want for a fling.
''Women make very good use of any information they get from a man's face,'' said co-author Dario Maestripieri, an associate professor of comparative human development at the University of Chicago. ''Depending on what they want and where they are in their lives, they use this information differently.''
In the study, published in Proceedings of the Royal Society B: Biological Sciences, researchers looked at a group of 39 men, ages 18 to 33, at the University of Chicago. Each man was shown 10 pairs of photographs and silhouettes, one of an adult and the other of an infant, and asked to rate their preferences. Meanwhile, their saliva was tested to determine testosterone levels.
Photographs of the men's faces were then shown to 29 women, ages 18 to 20, at the University of California at Santa Barbara.
The women were asked to rate the men on four qualities: ''likes children,'' ''masculine,'' ''physically attractive'' and ''kind.'' Then they were asked to rate how attractive they found each man for short-term and long-term romance.
The study found women did well at rating men on their interest in babies, and those they rated masculine generally had higher testosterone levels than the others.
For example, the men who indicated they liked children the most were rated as above average in liking children by 20 of the 29 women. The men who showed no interest in children were correctly rated as below average in that category by 19 of the women.
The higher the women rated the men for masculinity, the higher they were rated as potential short-term romantic partners. The higher they rated men for their interest in children, the higher they were rated for long-term romance.
The features that research has suggested denote high testosterone levels include a prominent jaw and a heavy beard.
The findings came as no surprise to those in the business of studying human behavior -- and love.
''What this study illustrates is that there are genetic programs that increase survival of the species because there are hormones in women that are cuing their reactions to the hormones of the men,'' said Dr. Daniel Alkon, scientific director of the Blanchette Rockefeller Neurosciences Institute in Morgantown, W.Va., and Washington.
Or as Kristin Kelly, a spokeswoman for the online dating service Match.com, put it: ''They call it `love at first sight' for a reason. They don't say `love at first sentence,' `love at first word.'''
It is unclear just what about the men's faces tipped the women off about their interest in children. While Maestripieri guessed it might have something to do with ''a more rounded face, a gentler face,'' Roney said the answer might be found in the expressions on the men's faces.
He explained that after the study was completed, five graduate students were asked to rate on a scale of 1 to 7 whether the men looked angry or happy. Though the men were instructed to have a neutral look on their faces when photographed, some apparently looked happier than others.
''It seemed that the men who picked more infants in that test had a happier or more content look on their face,'' he said.
Monday, May 08, 2006
It's expensive to live in California
NYTimes

May 7, 2006
The Least Affordable Place to Live? Try Salinas
By ALINA TUGEND
IN 2005, the least-affordable place in the country to live, measured by the percentage of income devoted to mortgage payments, was Salinas, Calif.
The second was the Santa Cruz-Watsonville area of California.
The third? Santa Rosa-Petaluma, Calif.
In fact, California has the distinction of having the 11 least-affordable metropolitan areas in the country. One would need to go all the way down to 12th place — and across the country to the New York region's northern suburbs — to find a non-California metropolitan area on the least-affordable list of 2005.
Much of California is pretty. It has beaches and the mountains and, of course, the weather. But why are places like Salinas, which is surrounded by agriculture, topping places like Honolulu (No. 17) and Miami (No. 22) on the out-of-reach list?
There is no one answer, but demographers and public planners who study such trends say that a confluence of factors in California — both artificial and natural — have combined to create a particularly acute problem.
"California has both political and geographical constraints on building," said Dowell Myers, professor of policy, planning and development at the University of Southern California. "That drives up prices, and then it snowballs."
The geographical limits on developable land are the hills and the coast, while the political restrictions are state and local regulations that prevent building new homes, in response to both environmental and congestion concerns.
"One of the key factors here is the basic law of supply and demand," said James W. Hughes, dean of the Edward J. Bloustein School of Planning and Public Policy at Rutgers University. "California is in marked contrast to Florida, where you can expand without constraint. It's more like the New York suburbs, where too many dollars are chasing too few homes."
While many states have regulations on growth, California is a leader, Dean Hughes says.
California is also in the forefront of population growth, but it is not driven, as might be expected, by envious Easterners and Midwesterners escaping snowbound winters. Nor is it driven by long-term Californians. In fact, census figures show that over the past decade, more people have left California — emigrating to neighboring states like Nevada and Arizona and farther away, to Texas and Florida — than have moved in from other parts of the country.
The population increase is driven primarily by births and foreign immigration. According to census statistics, from April 2000 to July 2005, California experienced a net natural increase — taking into account births and deaths — of 1.5 million people.
And an additional 1.4 million moved in from other countries.
While California's birth rate is not the highest in the nation — Utah's is — it is near the top.
"New York has the constraints but doesn't have the population growth," Professor Myers said. "Florida has the population growth but doesn't have the constraints."
While it is difficult to build new houses in California, that isn't to say none are going up. According to the California Association of Realtors, there have been increases in the number of housing units built over the past nine years — from 94,283 in 1996 to 207,154 in 2005.
That is substantially more than the low in 1993, when California was in the throes of a severe economic recession and only 84,656 units were built. But it's not as prolific as in 1988, when 255,559 went up.
There are a number of reasons for the restraints on home building, including the fact that many desirable areas in the state are already "built out" and the permit process is more complex and drawn out now than it was a few decades ago.
Leslie Appleton-Young, chief economist for the Realtors group, said the state needs about 250,000 units a year to meet housing demand. "We've been below that every year over the past 10 years," she said.
The high demand and low supply created a perfect breeding ground for investors and speculators, which became "the last straw" in driving housing prices up, said David Seiders, chief economist for the National Association of Home Builders.
Another quintessentially California issue is Proposition 13, the 1978 measure that slashed property taxes by more than 50 percent and ignited a national property tax revolution.
The measure, which was supposed to facilitate home buying, has backfired to some extent; local governments prefer that land be used for retailing rather than housing because they collect more from sales taxes than from property taxes.
"Proposition 13 is a big stop sign saying 'no housing needed,' " said Peter Dreier, professor of public policy at Occidental College in Los Angeles and an author of "Place Matters: Metropolitics for the 21st Century" (University Press of Kansas, 2001). "Every municipality is engaged in a bidding war for retail — they're battling for Wal-Mart, to keep the libraries open."
It is unlikely that will change, Professor Dreier and others say, calling Proposition 13 "the third rail of government — it's untouchable."
Although it is no surprise that house prices have gone through the roof in places like Los Angeles, San Diego and San Francisco, what is more unexpected is that less-popular areas away from the coast are also topping the list of least-affordable places to live.
"There's a huge movement away from L.A. County and from San Francisco and the great beneficiary is the Inland Empire" in Southern California, and in Sacramento and points east in northern California, said William Frey, a demographer at the Brookings Institution.
The migration is happening both among high-skilled and middle-class residents, as well as low-skilled and lower-class ones, so the cost of housing is exploding even in areas of the state that most people do not think of as traditionally expensive, he said.
"Baby boomers are getting older and moving into the higher-income bracket and into the top-dollar markets," Professor Myers said. "Immigrants have high ownership rates at the bottom of the market. It's a recipe for a bubble."
These noncoastal communities are no longer simply attached to established cities, but in many cases have become job centers in their own right, Ms. Appleton-Young said.
The Inland Empire, made up of Riverside and San Bernardino Counties, has been in a 30-year transition from a bedroom suburb to a metropolitan area, she said.
"People are now working where they live," Ms. Appleton-Young said. "It's not a commuter area."
The San Joaquin Valley, in central California, on the other hand, still has a way to go to attract an educated work force and to create a diverse and thriving economy. But Ms. Appleton-Young said it appears to be following in the footsteps of the Inland Empire: "As we say, jobs follow housing."
The final paradox in this state of paradoxes is that traditionally, many Californians are not homeowners; the state ranks 48th, behind only New York and Hawaii, in terms of homeownership, and about 10 percent below the national average. But over the past several years, even as housing prices have increased, more people are buying.
Home sales climbed fairly steadily from 1996 through 2005, with only a slight downward blip in 2001, said the California Realtors' association.
Hans Johnson, a demographer with the nonprofit Public Policy Institute of California, said, "It's counterintuitive." But apparently typical. Those familiar with home-purchasing trends say that people buy when the market is going up, not when it is going down.
If houses are so costly, how are people managing to make the leap and become homeowners?
In some cases, they use methods of financing that were not previously available, Mr. Johnson said. Instead of fixed-rate 30-year mortgages, they take, for example, variable-rate interest-only loans, which have lower monthly payments.
In many cases, he said, homeowners are paying far more on mortgages than the 30 percent of income recommended by the Department of Housing and Urban Development.
A study by the Public Policy Institute of California found that 40 percent of all households in California, the most anywhere, exceeded this recommended threshold. "In some cases, they're even paying more than half," Mr. Johnson said.
New homeowners are buying smaller homes or condominiums; according to the study, only 15 percent of long-term homeowners in California live in multifamily housing units, like condominiums, while 26 percent of recent buyers do.
"In some ways it's good, because people own a house and have equity," he said. "In other ways it's bad," he explained, because "if interest rates go up, there will be a large increase in monthly rates."
"If there's a bubble that bursts or slowly leaks," he added, overextended owners may not be able to sell and recover enough to pay off the loan.
Professor Dreier of Occidental College said he also blamed state government and business leaders for failing to support the creation of moderate-priced housing — not just for low-income residents, but also for middle-class people, like teachers and nurses, who cannot buy into the overheated housing market.
When he was a city official in Boston, the state government, businessmen and bankers "understood that affordable housing was part of a healthy work force," Professor Dreier said. "In California, businesses and the Chambers of Commerce have not embraced housing issues like they have embraced other issues, such as health care. We won't see the political will to solve the housing crisis until the organized business community weighs in and says it's unacceptable."
The big question now is whether the housing market will deflate while the economy stays strong, which would enable more Californians to buy. The answer seems as elusive as predicting the next earthquake.
The signs point toward a slowdown: interest rates are going up, and investors and speculators, who drove up prices by buying and selling houses, seem to be pulling back in hot markets nationally. But everyone, even those who study the subject, knows it is dangerous to predict.
Ask Professor Myers of U.S.C., who sold his house in Los Angeles last year. "I was convinced it was going to peak," he said. "After I sold, it rose another 15 percent."
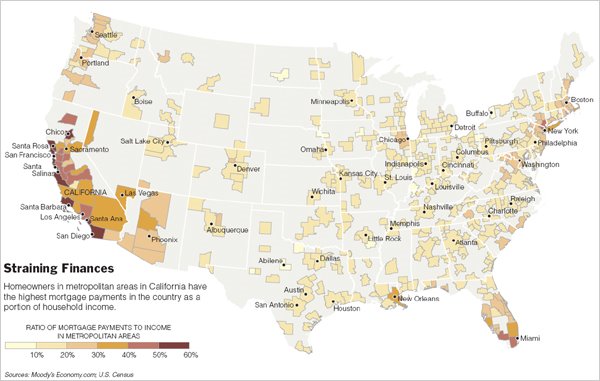
May 7, 2006
The Least Affordable Place to Live? Try Salinas
By ALINA TUGEND
IN 2005, the least-affordable place in the country to live, measured by the percentage of income devoted to mortgage payments, was Salinas, Calif.
The second was the Santa Cruz-Watsonville area of California.
The third? Santa Rosa-Petaluma, Calif.
In fact, California has the distinction of having the 11 least-affordable metropolitan areas in the country. One would need to go all the way down to 12th place — and across the country to the New York region's northern suburbs — to find a non-California metropolitan area on the least-affordable list of 2005.
Much of California is pretty. It has beaches and the mountains and, of course, the weather. But why are places like Salinas, which is surrounded by agriculture, topping places like Honolulu (No. 17) and Miami (No. 22) on the out-of-reach list?
There is no one answer, but demographers and public planners who study such trends say that a confluence of factors in California — both artificial and natural — have combined to create a particularly acute problem.
"California has both political and geographical constraints on building," said Dowell Myers, professor of policy, planning and development at the University of Southern California. "That drives up prices, and then it snowballs."
The geographical limits on developable land are the hills and the coast, while the political restrictions are state and local regulations that prevent building new homes, in response to both environmental and congestion concerns.
"One of the key factors here is the basic law of supply and demand," said James W. Hughes, dean of the Edward J. Bloustein School of Planning and Public Policy at Rutgers University. "California is in marked contrast to Florida, where you can expand without constraint. It's more like the New York suburbs, where too many dollars are chasing too few homes."
While many states have regulations on growth, California is a leader, Dean Hughes says.
California is also in the forefront of population growth, but it is not driven, as might be expected, by envious Easterners and Midwesterners escaping snowbound winters. Nor is it driven by long-term Californians. In fact, census figures show that over the past decade, more people have left California — emigrating to neighboring states like Nevada and Arizona and farther away, to Texas and Florida — than have moved in from other parts of the country.
The population increase is driven primarily by births and foreign immigration. According to census statistics, from April 2000 to July 2005, California experienced a net natural increase — taking into account births and deaths — of 1.5 million people.
And an additional 1.4 million moved in from other countries.
While California's birth rate is not the highest in the nation — Utah's is — it is near the top.
"New York has the constraints but doesn't have the population growth," Professor Myers said. "Florida has the population growth but doesn't have the constraints."
While it is difficult to build new houses in California, that isn't to say none are going up. According to the California Association of Realtors, there have been increases in the number of housing units built over the past nine years — from 94,283 in 1996 to 207,154 in 2005.
That is substantially more than the low in 1993, when California was in the throes of a severe economic recession and only 84,656 units were built. But it's not as prolific as in 1988, when 255,559 went up.
There are a number of reasons for the restraints on home building, including the fact that many desirable areas in the state are already "built out" and the permit process is more complex and drawn out now than it was a few decades ago.
Leslie Appleton-Young, chief economist for the Realtors group, said the state needs about 250,000 units a year to meet housing demand. "We've been below that every year over the past 10 years," she said.
The high demand and low supply created a perfect breeding ground for investors and speculators, which became "the last straw" in driving housing prices up, said David Seiders, chief economist for the National Association of Home Builders.
Another quintessentially California issue is Proposition 13, the 1978 measure that slashed property taxes by more than 50 percent and ignited a national property tax revolution.
The measure, which was supposed to facilitate home buying, has backfired to some extent; local governments prefer that land be used for retailing rather than housing because they collect more from sales taxes than from property taxes.
"Proposition 13 is a big stop sign saying 'no housing needed,' " said Peter Dreier, professor of public policy at Occidental College in Los Angeles and an author of "Place Matters: Metropolitics for the 21st Century" (University Press of Kansas, 2001). "Every municipality is engaged in a bidding war for retail — they're battling for Wal-Mart, to keep the libraries open."
It is unlikely that will change, Professor Dreier and others say, calling Proposition 13 "the third rail of government — it's untouchable."
Although it is no surprise that house prices have gone through the roof in places like Los Angeles, San Diego and San Francisco, what is more unexpected is that less-popular areas away from the coast are also topping the list of least-affordable places to live.
"There's a huge movement away from L.A. County and from San Francisco and the great beneficiary is the Inland Empire" in Southern California, and in Sacramento and points east in northern California, said William Frey, a demographer at the Brookings Institution.
The migration is happening both among high-skilled and middle-class residents, as well as low-skilled and lower-class ones, so the cost of housing is exploding even in areas of the state that most people do not think of as traditionally expensive, he said.
"Baby boomers are getting older and moving into the higher-income bracket and into the top-dollar markets," Professor Myers said. "Immigrants have high ownership rates at the bottom of the market. It's a recipe for a bubble."
These noncoastal communities are no longer simply attached to established cities, but in many cases have become job centers in their own right, Ms. Appleton-Young said.
The Inland Empire, made up of Riverside and San Bernardino Counties, has been in a 30-year transition from a bedroom suburb to a metropolitan area, she said.
"People are now working where they live," Ms. Appleton-Young said. "It's not a commuter area."
The San Joaquin Valley, in central California, on the other hand, still has a way to go to attract an educated work force and to create a diverse and thriving economy. But Ms. Appleton-Young said it appears to be following in the footsteps of the Inland Empire: "As we say, jobs follow housing."
The final paradox in this state of paradoxes is that traditionally, many Californians are not homeowners; the state ranks 48th, behind only New York and Hawaii, in terms of homeownership, and about 10 percent below the national average. But over the past several years, even as housing prices have increased, more people are buying.
Home sales climbed fairly steadily from 1996 through 2005, with only a slight downward blip in 2001, said the California Realtors' association.
Hans Johnson, a demographer with the nonprofit Public Policy Institute of California, said, "It's counterintuitive." But apparently typical. Those familiar with home-purchasing trends say that people buy when the market is going up, not when it is going down.
If houses are so costly, how are people managing to make the leap and become homeowners?
In some cases, they use methods of financing that were not previously available, Mr. Johnson said. Instead of fixed-rate 30-year mortgages, they take, for example, variable-rate interest-only loans, which have lower monthly payments.
In many cases, he said, homeowners are paying far more on mortgages than the 30 percent of income recommended by the Department of Housing and Urban Development.
A study by the Public Policy Institute of California found that 40 percent of all households in California, the most anywhere, exceeded this recommended threshold. "In some cases, they're even paying more than half," Mr. Johnson said.
New homeowners are buying smaller homes or condominiums; according to the study, only 15 percent of long-term homeowners in California live in multifamily housing units, like condominiums, while 26 percent of recent buyers do.
"In some ways it's good, because people own a house and have equity," he said. "In other ways it's bad," he explained, because "if interest rates go up, there will be a large increase in monthly rates."
"If there's a bubble that bursts or slowly leaks," he added, overextended owners may not be able to sell and recover enough to pay off the loan.
Professor Dreier of Occidental College said he also blamed state government and business leaders for failing to support the creation of moderate-priced housing — not just for low-income residents, but also for middle-class people, like teachers and nurses, who cannot buy into the overheated housing market.
When he was a city official in Boston, the state government, businessmen and bankers "understood that affordable housing was part of a healthy work force," Professor Dreier said. "In California, businesses and the Chambers of Commerce have not embraced housing issues like they have embraced other issues, such as health care. We won't see the political will to solve the housing crisis until the organized business community weighs in and says it's unacceptable."
The big question now is whether the housing market will deflate while the economy stays strong, which would enable more Californians to buy. The answer seems as elusive as predicting the next earthquake.
The signs point toward a slowdown: interest rates are going up, and investors and speculators, who drove up prices by buying and selling houses, seem to be pulling back in hot markets nationally. But everyone, even those who study the subject, knows it is dangerous to predict.
Ask Professor Myers of U.S.C., who sold his house in Los Angeles last year. "I was convinced it was going to peak," he said. "After I sold, it rose another 15 percent."
Sunday, May 07, 2006
Tracking prescribing data
NYTimes
May 4, 2006
Doctors Object to Gathering of Drug Data
By STEPHANIE SAUL
Although virtually unknown to consumers, the information has long been considered the most potent weapon in pharmaceutical sales — computerized dossiers showing which physicians are prescribing what drugs. Armed with such data, a drug sales representative can pressure a doctor to write more prescriptions for a name-brand medicine or fewer orders for a competitor's drug.
But now a rebellion is under way by some doctors, who consider the data-gathering an intrusion that feeds overzealous sales practices among the nation's estimated 90,000 drug company representatives. Public officials are also weighing in. A vote on a state bill to clamp down on the practice is scheduled for today in New Hampshire, and similar bills have been introduced in other states, including Arizona and West Virginia.
To appease the doctors and try to stave off the state restrictions, the American Medical Association will soon give individual physicians the choice of declaring their prescription records off limits to drug sales representatives. The new measure is viewed as a self-policing move that the drug industry and the A.M.A., which has lucrative contracts with data-mining companies, hope will keep states from banning sales of prescription data altogether.
If the A.M.A effort succeeds, "legislators will turn their attention elsewhere, and the industry can hang on to one of its most valuable data sources," according to an article this week in the industry trade magazine Pharmaceutical Executive, which was co-written by an A.M.A. official and an executive with the leading vendor of prescription data. Even many critics concede that patients' privacy is apparently not an issue, because the tracking systems identify only the prescribing doctors, not patients. But many doctors find the use of the data by sales representatives an intrusion into the way they practice medicine.
"These doctors were outraged that people came into their office and talked to them about how many times they prescribed a particular drug," said Dr. John C. Lewin, the chief executive of the state medical association in California, one of the states where complaints about the current system arose.
The California group is beginning its own program under which doctors who do not opt out under the A.M.A. system will get comparisons of their prescribing patterns in 17 classes of drugs from the data companies, said Dr. Lewin, who added that the program was being started as a pilot effort that he hoped would be extended statewide.
Among the doctors who raised an early complaint about the system was Dr. Brad Drexler, an obstetrician in Healdsburg, Calif., who said he was surprised four years ago when pharmaceutical representatives began thanking him for writing prescriptions — the first time he realized that the drug representatives had information he assumed was private.
"I think it adds to the potential that physicians could be targeted one way or another for perks," said Dr. Drexler, alluding to the practice by drug companies of deciding which doctors to reward with the gifts, meals and other perks that sales representatives have dangled over the years, or to gauge which physicians might be worthy of signing up as paid speakers or consultants.
"It's the most powerful tool a drug rep has, for sure," said Jamie Reidy, a former drug salesman who was fired last year by Eli Lilly & Company after writing "Hard Sell," a humorous exposé of the pharmaceutical industry. Mr. Reidy said the pharmaceutical representatives received updated prescription data every two weeks. The information also sometimes characterizes each physician's prescribing patterns, Mr. Reidy said.
For example, "early prescribers" — also known among drug representatives as "cowboys," according to Mr. Reidy — are those doctors who start prescribing a drug as soon as it comes to market. If you are a drug sales representative, "you go to see that doctor in the first week," Mr. Reidy said.
Although the drug representatives are told not to share the prescribing details with doctors, some nonetheless have confronted doctors with the data. A representative might become frustrated, for example, if after providing numerous lunches to a doctor's staff, the data show that the doctor is not writing prescriptions for the company's drug.
"It just creates a weird atmosphere," Mr. Reidy said.
State Representative Cindy Rosenwald of New Hampshire, lead sponsor of her state's bill, said she was motivated partly by high Medicaid drug costs, which she said she believed had been driven up by the pharmaceutical industry's success in coaxing doctors to prescribe expensive brand-name drugs.
"To me this is a money issue," Ms. Rosenwald said. "When I look at our state's budget, the fastest-growing part of the Medicaid program here in New Hampshire is for prescription drugs. It's an enormous cost for a small state like New Hampshire."
Ms. Rosenwald's legislation has been adopted by the New Hampshire House and is tentatively set for a Senate vote this afternoon.
She said she did not believe the A.M.A.'s self-policing measure would provide enough protection, partly because even if doctors specify that their prescription records not be available to drug sales representatives, the information would still be sold to drug companies for other marketing and research purposes. The drug companies, she said, would be on their honor not to share the data with their sales staffs. A Gallup Poll commissioned by the A.M.A. in 2004 found that two-thirds of doctors surveyed were opposed to the release of such data to pharmaceutical representatives, and that 77 percent felt that an opt-out program would alleviate concerns about the release of data. Nearly a quarter of the doctors were not even aware that the pharmaceutical industry had access to such information.
That same year, the American College of Physicians requested that the A.M.A. prohibit the release or sale of doctors' prescribing information. The college represents internists and related medical subspecialties, while the A.M.A. is a broader trade group whose members include all doctors, including surgeons.
Dr. Dean Abramson, an Iowa physician, is among the doctors who plan to opt out under the new A.M.A. process, which will involve a sign-up registry that goes into use on July 1. His opposition began nearly a decade ago, he recalled, when a representative from TAP Pharmaceutical Products let slip during a sales call that Dr. Abramson wrote more prescriptions for Prevacid, a treatment for acid reflux, than any other doctor in the state.
"I was pretty surprised that they kept that data, and I was not happy at all," Dr. Abramson said. "I said, 'Why is that data even kept?' She didn't really give me an answer."
Since then, Dr. Abramson has become something of an activist against the lunches and gifts that the pharmaceutical industry dispenses to doctors. His gastroenterology group in Cedar Rapids, Iowa, accepts neither, he said.
The leading compiler and vendor of prescription data is IMS Health, a publicly traded company based in Fairfield, Conn., that had revenue last year of $1.75 billion. IMS and its competitors gather the data through contracts with retail pharmacy chains and companies that manage drug plans for insurers, then sell it to pharmaceutical companies.
IMS and its competitors — the main ones are Verispan, Dendrite International and a Dutch company, Wolters Kluwer — also pay the A.M.A. for access to its repository of information on approximately one million doctors who are graduates of American medical schools, as well as foreign medical school graduates licensed in the United States.
The A.M.A., which calls this repository Masterfile, begins collecting the information when a doctor enters medical school. Over doctors' careers, additional material includes information on their board certifications, types of practice and disciplinary records. The Masterfile information is among data that companies like IMS use in developing physician profiles.
In an interview, IMS officials said they believed that state efforts to curtail their activities were misguided. "Limiting the access to our data will not stop pharmaceutical marketing," said Robert J. Hunkler, whose job with the company includes serving as a liaison with the medical profession. Mr. Hunkler also says that the data his company collects is valuable for medical research and is sometimes shared free with researchers.
Mr. Hunkler was a co-author of the Pharmaceutical Executive article describing the new A.M.A. program. The other writer was Robert A. Musacchio, the A.M.A.'s senior vice president for publishing and business services. While Mr. Musacchio declined to disclose the exact value of its Masterfile contracts with the four main data companies, he said that the organization made $40 million a year selling information, which also includes mailing lists and a service through which hospitals can check the credentials of doctors. Mr. Musacchio said that doctors had always been able to put a "no contact" status on their Masterfile record, meaning their name would not be licensed for marketing by mail, telephone or fax.
The A.M.A.'s new registry, administered partly through a Web site, will enable doctors listed in its Masterfile to indicate that they do not want their prescribing data shared with pharmaceutical sales representatives. The decision will remain in force for three years.
And yet, even those doctors' prescription information will still be collected and transmitted to drug companies, whose other uses of the data include tallying bonuses paid to pharmaceutical representatives, which are based on sales. "What we've always stressed is that physicians have rights and they can always tell pharmaceutical representatives that they don't want to be called upon," said Mr. Musacchio. But he said the organization had always made clear to the pharmaceutical industry that its representatives should never "badger or embarrass or harass" physicians.
"They sometimes try to get their point across a little too strongly," he said.
May 4, 2006
Doctors Object to Gathering of Drug Data
By STEPHANIE SAUL
Although virtually unknown to consumers, the information has long been considered the most potent weapon in pharmaceutical sales — computerized dossiers showing which physicians are prescribing what drugs. Armed with such data, a drug sales representative can pressure a doctor to write more prescriptions for a name-brand medicine or fewer orders for a competitor's drug.
But now a rebellion is under way by some doctors, who consider the data-gathering an intrusion that feeds overzealous sales practices among the nation's estimated 90,000 drug company representatives. Public officials are also weighing in. A vote on a state bill to clamp down on the practice is scheduled for today in New Hampshire, and similar bills have been introduced in other states, including Arizona and West Virginia.
To appease the doctors and try to stave off the state restrictions, the American Medical Association will soon give individual physicians the choice of declaring their prescription records off limits to drug sales representatives. The new measure is viewed as a self-policing move that the drug industry and the A.M.A., which has lucrative contracts with data-mining companies, hope will keep states from banning sales of prescription data altogether.
If the A.M.A effort succeeds, "legislators will turn their attention elsewhere, and the industry can hang on to one of its most valuable data sources," according to an article this week in the industry trade magazine Pharmaceutical Executive, which was co-written by an A.M.A. official and an executive with the leading vendor of prescription data. Even many critics concede that patients' privacy is apparently not an issue, because the tracking systems identify only the prescribing doctors, not patients. But many doctors find the use of the data by sales representatives an intrusion into the way they practice medicine.
"These doctors were outraged that people came into their office and talked to them about how many times they prescribed a particular drug," said Dr. John C. Lewin, the chief executive of the state medical association in California, one of the states where complaints about the current system arose.
The California group is beginning its own program under which doctors who do not opt out under the A.M.A. system will get comparisons of their prescribing patterns in 17 classes of drugs from the data companies, said Dr. Lewin, who added that the program was being started as a pilot effort that he hoped would be extended statewide.
Among the doctors who raised an early complaint about the system was Dr. Brad Drexler, an obstetrician in Healdsburg, Calif., who said he was surprised four years ago when pharmaceutical representatives began thanking him for writing prescriptions — the first time he realized that the drug representatives had information he assumed was private.
"I think it adds to the potential that physicians could be targeted one way or another for perks," said Dr. Drexler, alluding to the practice by drug companies of deciding which doctors to reward with the gifts, meals and other perks that sales representatives have dangled over the years, or to gauge which physicians might be worthy of signing up as paid speakers or consultants.
"It's the most powerful tool a drug rep has, for sure," said Jamie Reidy, a former drug salesman who was fired last year by Eli Lilly & Company after writing "Hard Sell," a humorous exposé of the pharmaceutical industry. Mr. Reidy said the pharmaceutical representatives received updated prescription data every two weeks. The information also sometimes characterizes each physician's prescribing patterns, Mr. Reidy said.
For example, "early prescribers" — also known among drug representatives as "cowboys," according to Mr. Reidy — are those doctors who start prescribing a drug as soon as it comes to market. If you are a drug sales representative, "you go to see that doctor in the first week," Mr. Reidy said.
Although the drug representatives are told not to share the prescribing details with doctors, some nonetheless have confronted doctors with the data. A representative might become frustrated, for example, if after providing numerous lunches to a doctor's staff, the data show that the doctor is not writing prescriptions for the company's drug.
"It just creates a weird atmosphere," Mr. Reidy said.
State Representative Cindy Rosenwald of New Hampshire, lead sponsor of her state's bill, said she was motivated partly by high Medicaid drug costs, which she said she believed had been driven up by the pharmaceutical industry's success in coaxing doctors to prescribe expensive brand-name drugs.
"To me this is a money issue," Ms. Rosenwald said. "When I look at our state's budget, the fastest-growing part of the Medicaid program here in New Hampshire is for prescription drugs. It's an enormous cost for a small state like New Hampshire."
Ms. Rosenwald's legislation has been adopted by the New Hampshire House and is tentatively set for a Senate vote this afternoon.
She said she did not believe the A.M.A.'s self-policing measure would provide enough protection, partly because even if doctors specify that their prescription records not be available to drug sales representatives, the information would still be sold to drug companies for other marketing and research purposes. The drug companies, she said, would be on their honor not to share the data with their sales staffs. A Gallup Poll commissioned by the A.M.A. in 2004 found that two-thirds of doctors surveyed were opposed to the release of such data to pharmaceutical representatives, and that 77 percent felt that an opt-out program would alleviate concerns about the release of data. Nearly a quarter of the doctors were not even aware that the pharmaceutical industry had access to such information.
That same year, the American College of Physicians requested that the A.M.A. prohibit the release or sale of doctors' prescribing information. The college represents internists and related medical subspecialties, while the A.M.A. is a broader trade group whose members include all doctors, including surgeons.
Dr. Dean Abramson, an Iowa physician, is among the doctors who plan to opt out under the new A.M.A. process, which will involve a sign-up registry that goes into use on July 1. His opposition began nearly a decade ago, he recalled, when a representative from TAP Pharmaceutical Products let slip during a sales call that Dr. Abramson wrote more prescriptions for Prevacid, a treatment for acid reflux, than any other doctor in the state.
"I was pretty surprised that they kept that data, and I was not happy at all," Dr. Abramson said. "I said, 'Why is that data even kept?' She didn't really give me an answer."
Since then, Dr. Abramson has become something of an activist against the lunches and gifts that the pharmaceutical industry dispenses to doctors. His gastroenterology group in Cedar Rapids, Iowa, accepts neither, he said.
The leading compiler and vendor of prescription data is IMS Health, a publicly traded company based in Fairfield, Conn., that had revenue last year of $1.75 billion. IMS and its competitors gather the data through contracts with retail pharmacy chains and companies that manage drug plans for insurers, then sell it to pharmaceutical companies.
IMS and its competitors — the main ones are Verispan, Dendrite International and a Dutch company, Wolters Kluwer — also pay the A.M.A. for access to its repository of information on approximately one million doctors who are graduates of American medical schools, as well as foreign medical school graduates licensed in the United States.
The A.M.A., which calls this repository Masterfile, begins collecting the information when a doctor enters medical school. Over doctors' careers, additional material includes information on their board certifications, types of practice and disciplinary records. The Masterfile information is among data that companies like IMS use in developing physician profiles.
In an interview, IMS officials said they believed that state efforts to curtail their activities were misguided. "Limiting the access to our data will not stop pharmaceutical marketing," said Robert J. Hunkler, whose job with the company includes serving as a liaison with the medical profession. Mr. Hunkler also says that the data his company collects is valuable for medical research and is sometimes shared free with researchers.
Mr. Hunkler was a co-author of the Pharmaceutical Executive article describing the new A.M.A. program. The other writer was Robert A. Musacchio, the A.M.A.'s senior vice president for publishing and business services. While Mr. Musacchio declined to disclose the exact value of its Masterfile contracts with the four main data companies, he said that the organization made $40 million a year selling information, which also includes mailing lists and a service through which hospitals can check the credentials of doctors. Mr. Musacchio said that doctors had always been able to put a "no contact" status on their Masterfile record, meaning their name would not be licensed for marketing by mail, telephone or fax.
The A.M.A.'s new registry, administered partly through a Web site, will enable doctors listed in its Masterfile to indicate that they do not want their prescribing data shared with pharmaceutical sales representatives. The decision will remain in force for three years.
And yet, even those doctors' prescription information will still be collected and transmitted to drug companies, whose other uses of the data include tallying bonuses paid to pharmaceutical representatives, which are based on sales. "What we've always stressed is that physicians have rights and they can always tell pharmaceutical representatives that they don't want to be called upon," said Mr. Musacchio. But he said the organization had always made clear to the pharmaceutical industry that its representatives should never "badger or embarrass or harass" physicians.
"They sometimes try to get their point across a little too strongly," he said.
American Idol beginnings
NYTimes
April 30, 2006
How a Hit Almost Failed Its Own Audition
By BILL CARTER
Network television programmers face a challenging job, though not a complicated one: they need to find hits. That's why they spend millions to find and hire talented writers, actors and producers. In many cases they would be wiser to invest in a catcher's mitt, because really big hits, ones that can transform the fates of networks — and of network executives — tend to fall from the sky. Here is the story of how "American Idol," the biggest hit on television, hovered over every network in 2001, waiting for one of them to grab it. This article is adapted from "Desperate Networks" by Bill Carter, a reporter for The New York Times. Doubleday will publish the book on Tuesday.
SIMON COWELL sat at a meeting in Los Angeles with executives from someplace he had never heard of, something called the UPN network. Mr. Cowell, a British music executive, had never pitched a television show in America before — and the way things were going, he felt as though he never would again.
The UPN executives who sat across the table from Mr. Cowell at that meeting in April 2001 clearly had no clue who this guy was, and, apparently, even less interest in finding out. Maybe they knew his business partner, Simon Fuller, from his leadership of the Spice Girls. Surely, they had heard of the Spice Girls. But, then again, as Mr. Cowell checked those blank, uninterested faces, maybe not.
No matter. Mr. Cowell had enormous faith in the idea that he and Mr. Fuller had for a music-based television show. Mr. Fuller was the most successful manager of music acts in Britain and he, Mr. Cowell, was the most successful artist and repertoire man — that is, music label talent manager — currently working there. They both knew how to launch new singing artists, and now they had an idea for a show that would allow them to utilize their talents on camera.
Despite the wall he sensed going up at the UPN meeting, Mr. Cowell, never cowed, simply plowed ahead with his pitch. "What this is really about is the American dream," Mr. Cowell told the American executives in his smooth British tones. He laid out the format for the show that he and Mr. Fuller were calling "Pop Idol" in Britain, describing how exciting this show would surely be. When Mr. Cowell wrapped up his comments, the room went quiet — stone silent.
At the opposite end of the table, a young woman executive, whom Mr. Cowell had identified in his head as the "lippy second-in-command," seemed to be calculating whether or not this truly was the end of the presentation.
"And what exactly do you think we're supposed to be doing for you?" the woman said, dismissively.
"Well, actually, sweetheart," Mr. Cowell replied, applying just a dash of acid, "it's more a question of what I could be doing for you."
Again a terrible silence fell. Then the woman piped up: "Well, we'll get back to you."
Mr. Cowell said he had heard that line before — too many times for it to bother him during his sojourn in the United States trying to spark some American interest in this hot idea. He and Mr. Fuller and a third partner, yet another Simon — Simon Jones, an executive with Thames Television — had paid calls to the broadcast networks, to MTV and to other cable networks. Every one of them had a free shot that April at landing the show that the three Simons were putting on offer. No one showed the least interest, and many of the network executives offered shoulders so cold that Mr. Cowell could have chilled his wine on them. Uniformly, they had been, Mr. Cowell was convinced, the worst, most appalling meetings of his life.
The contrast with how "Pop Idol" had been sold in Britain could not have been sharper. Mr. Cowell and Mr. Fuller met with representatives of the British network ITV, spent what Mr. Cowell estimated was no more than 30 seconds describing the idea, and they had a deal. But, of course, the two Simons had enormous reputations in the British entertainment world, and they were entering a market that had already embraced music-oriented reality shows.
In Britain, "Pop Stars," a show that was originally developed in Australia and traced the formation of a singing group, had engrossed the nation. Another music show, "Fame Academy," had also done extremely well.
Mr. Cowell had been invited to be a judge on the first edition of "Pop Stars," and, at first, had accepted. But he quickly had misgivings about being a person who ran a music label going on television to demonstrate how to put together a group. Mr. Cowell thought it was "like a magician showing how you saw somebody in half." He bowed out.
When Mr. Cowell got a first glimpse of "Pop Stars," however, he knew he had made a mistake. The show looked like a piping hot hit to him — though he had an instant insight. To him, the attractive part of "Pop Stars" was the round of auditions to select the band members. He thought that, as constituted, "Pop Stars" had no ending. With Mr. Fuller he conceived a show built around seasonlong tryouts with the winner announced at the end.
What Mr. Cowell told ITV was this: "It will have all the fun of 'Pop Stars,' but we can do it better. We can do it a lot harsher than on 'Pop Stars,' and the public will vote and choose the winner. And we won't be relying on the music to make the show successful: it will be a soap opera."
Mr. Cowell also volunteered himself as a judge, knowing that he had the precise expertise called for in selecting a singing star. Mr. Fuller and his company, 19 Entertainment, owned the show along with Fremantle Media, a big European production company. Mr. Cowell took no ownership stake, but he did get royalty rights for his label, Syco Records, a part of the BMG Music Group, on every recording released by an "Idol" performer worldwide. That was the essence of the show's appeal for Mr. Cowell.
All he was concerned with was that the right person would win, so that he would get access to a good artist. If the show was a hit, so much the better; Mr. Cowell's new artist was more likely to sell a lot of records that way.
When Mr. Cowell started shooting "Pop Idol" in England in the summer of 2001, the production plan called for four judges to sit in an audition room while contestants trooped in, one by one. The judges would discuss each singer after he or she left the room. Nothing more specific was spelled out.
The first auditions took place in Manchester. But by the time five or six singers had walked through, sung and then had their performances rehashed by the judges after they had left the room, Mr. Cowell was almost crawling up the walls.
"I'm dying in here," he told the producers. "This is not like a real-life audition." He turned to one of the other judges, the veteran British pop producer Pete Waterman, and said: "We have to actually tell the performers to their faces what we thought. We've just got to tell these boys and girls the truth. They're rubbish."
Mr. Cowell had invited Mr. Waterman to work as a judge, expecting him to be what Mr. Cowell described as the "nasty" one. But Mr. Waterman got more emotional on the show than Mr. Cowell expected. (It was published in the British press that he actually teared up at one performance). Mr. Cowell, meanwhile, acted no differently on the air than he did at real auditions — he was cold and distant. And his comments reflected that.
As the show took off after its premiere that October, the British press concentrated on Mr. Cowell and his barbed comments. He was the nasty one, the "mouthy" one. The show quickly began to revolve around Mr. Cowell and his withering appraisals of the wretched talent being brought before him.
"Pop Idol" was the hit of the year in Britain. The two finalists both released albums after the show concluded and sold millions of copies. Mr. Fuller had two new hit artists to manage; Mr. Cowell's label had two huge-selling albums. Their collaboration was a ringing success — and they were just getting started.
Alix Hartley, a British-born talent agent with an expertise in music, who worked for the Creative Artists Agency, the heavyweight Hollywood talent agency, was a natural to represent Mr. Fuller in the challenge of going back to the networks in the fall of 2001 and finding "Pop Idol" a home on American television.
Given how both "Who Wants to Be a Millionaire" and "Survivor" — both conceived by British producers — had emerged as hits on American television in the summer months, C.A.A.'s strategy was to pitch "Pop Idol" around as a perfect new reality programming vehicle for the summer of 2002. It was light, entertaining and not very expensive to produce. As an added advantage, having started a 15-week British run in October, it would have fully executed weekly editions on tape to serve as the template for the American version.
ANDREA WONG, who ran the reality-programming department for ABC, was an ideal target for the C.A.A. pitch. She was aggressively seeking reality programs and had been closely watching the British market in the wake of her network's failure to secure "Survivor" when it had twice been in ABC's clutches.
But C.A.A. and the producers of "Pop Idol" ran into a problem that "Survivor" never had to face. Music had already failed in the United States in reality formats on two networks, one being ABC.
That network tried a show in 2000 called "Making the Band," about assembling a boy-band singing group. Though it had a small following, mostly among pubescent girls, the show simply could not cross over into a wider audience. The music format was blamed. Music had become just too stratified, the argument went, to ever build a wide-enough appeal in the United States to succeed on the scale that an American network television show required.
The WB network, which was mainly the network of pubescent girls, tried a similar format the next season with a show that the network called "Pop Stars," a format derived from the Australian and British models of the same name — only with an-all girl group. It, too, found only a niche audience.
Ms. Wong knew all of that when C.A.A. came in touting "Pop Idol." She passed. C.A.A. next met with NBC's reality executives. They passed. The agency never set up a formal meeting with CBS's reality division, feeling as though an initial phone call to CBS had fallen utterly flat.
That left Fox. The British producers had gotten nowhere in the spring when they tried to interest Fox's reality division, headed by Mike Darnell, in "Pop Idol." But C.A.A. made a new effort anyway. This time Ms. Hartley of C.A.A. and Mr. Fuller — without Mr. Cowell this time — went in to see Mr. Darnell himself.
Mr. Fuller pitched his idea with fervent passion, and that impressed Mr. Darnell. He really liked the notion that the format would essentially be all audition, complete with a lot of really woeful early performances. Mr. Darnell had never liked the band-making shows once they got past the auditions. Here was a format in which the auditions, replete with people making cringe-inducing fools of themselves, would rule.
Mr. Darnell, thinking of summer budgets at Fox, wanted to know if the show had sponsorship attached. Ms. Hartley told him that C.A.A. was working on that very angle. Mr. Darnell told Ms. Hartley and Mr. Fuller that they should bring up the idea with Sandy Grushow, the head of entertainment for Fox, and his chief lieutenant, Gail Berman.
When Mr. Grushow and Ms. Berman heard the pitch, both had the same reaction: tepid. A talent contest did not sound like inspiring television in the 21st century — or like a breakout hit, for which Fox had an increasingly searing need at that point.
But both executives knew that the network could also use something that might pass for fresh summer programming. The problem was, Fox was out of money. The program budget for the year was exhausted, bone dry.
Mr. Grushow told the C.A.A. representatives that Fox was simply not going to pay a license fee for this program — if it was going to get on the air, it would have to be as a fully sponsored broadcast. "We don't know much about this show," Mr. Grushow told them. "But if we can get it for nothing, it's sort of a no-brainer."
C.A.A. indicated that, of course, it could line up sponsors. Fox said: Come back to us when you do.
By this point, early in winter, "Pop Idol" had become the talk of Britain. Fox had made no effort to secure the show, so C.A.A. went back to Ms. Wong from ABC, armed with those mighty ratings from the British run. She asked to see a tape of the British show. That was encouraging. A tape was delivered. Ms. Wong watched it — and passed again.
The impasse with Fox continued. C.A.A. heard nothing from Mr. Darnell. Ms. Berman and Mr. Grushow continued to press for a fully sponsored show; nothing was happening, despite the fabulous success in Britain.
But even as talks with Fox dragged on, C.A.A. was trying to exploit a connection that some at the agency believed might play out to their advantage. Back in October, several C.A.A. executives had met with Elisabeth Murdoch, daughter of Rupert Murdoch, the founder and chief executive of the News Corporation, which owns Fox. The meeting took place at Mipcom, the international television programming festival in Cannes, France. A blossoming relationship took hold there.
With the talks about "Idol" stalled in Los Angeles, the C.A.A. representatives at one point mentioned the show in a conversation with Ms. Murdoch, who ran the News Corporation's most important television operation in England, the BSkyB satellite channel. She, of course, was witnessing the phenomenon of "Pop Idol" firsthand, on her home TV set.
Fortunately for C.A.A., Ms. Murdoch flat-out loved the show. Hearing that her father's American network had yet to act on making a deal for the United States rights, she decided to give the process a helpful nudge. She called her father and told him how much she loved "Pop Idol" and how big the show was becoming in England. She urged him to buy the rights for Fox.
Mr. Murdoch put in a call the next day to Peter Chernin, his No. 2 at the News Corporation and the top decision-maker on all the biggest moves made by the Fox network. "What's going on with this show 'Pop Idol,' Peter?" Mr. Murdoch asked Mr. Chernin. "It's a big hit in England. I spoke to Liz and she says it's great."
Mr. Chernin was familiar enough with the situation to report that Fox's network people had been talking about it with the agency, discussing potential advertising backers. "We're still looking at it," he said.
Mr. Murdoch shot back: "Don't look at it. Buy it! Right now."
With those marching orders ringing in his ears, Mr. Chernin followed up quickly, calling Mr. Grushow and Ms. Berman. He asked them the status of "Pop Idol." They told him that they were still waiting for the advertiser sponsorships to come through.
"Just close the deal," Mr. Chernin said. He explained the call from Mr. Murdoch.
Mr. Grushow said, "We'll get it closed today."
The actual order for the series suddenly changed as well. Instead of an eight-episode summer order, Fox began asking C.A.A. for the rights to broadcast 15 episodes — the same duration as the show in Britain. The C.A.A. agents concluded that one of the Murdochs, or maybe both, had insisted that the show be done exactly as it was in England.
That did not mean that Fox would import the British hosts and judges. Fox fully expected to hire figures from the American music industry for those jobs. But after the deal was concluded, and Mr. Grushow finally was able to watch a tape of the British version, he told Ms. Berman that he was taken by the nastily charismatic figure on the British judging panel. "I think as part of the deal, we should insist on bringing this guy over as a judge," he said. At that point, he could not remember Simon Cowell's name.
"Pop Idol" made Mr. Cowell one of the most talked-about cultural figures in Britain in the winter of 2002. He was a tabloid newspaper's dream: seen by millions every week on television, saying something outrageously quotable ("You're a disaster"), doing something unconscionably cruel (several young women left the auditions convulsed in tears after hearing his corrosive assessments of their talents) and tirelessly promoting his program (by doing every sort of interview in print and on television and radio).
Mr. Cowell said he was pleased when he heard that the show had finally sold in the United States but mildly shocked when he learned that Fox was requesting that he come along to be a judge on the American version. He had not planned on turning himself into an international television star; he said he wanted only to make the show a hit for the benefit of his record label.
At first he had doubts about whether he knew enough about American music to judge American singers. He was also concerned because of the way American television executives functioned during those hideous meetings in the spring. He expected that some genius at the American network was bound to try to water down the show, and especially his honestly acerbic comments. He would have no interest in a sweetened version of "Pop Idol."
Then Kevin Warwick, one of the producers of the British show, called. "Look, Simon, we're going over to produce the show in America," he said. "I will look after your back again. You won't have to compromise what you do. You can be yourself."
Mr. Cowell asked, "So I can really be the same as I was in England?"
Mr. Warwick assured him that he could.
A few weeks later, Mr. Cowell arrived in Los Angeles for his first round of meetings with Fox and the American producer, Brian Gadinsky. At first they considered rechristening it "America's Idol." Mr. Darnell thought that made it sound as if it might be about a New York fireman, so he suggested "American Idol." (Nobody wanted "pop" in the title because nobody in the music business in the United States ever used the word "pop" anymore — with the exception of Michael Jackson — and because "Pop Stars" had been a failure for the WB network.)
Mr. Murdoch, as he often did, sat in on a meeting that winter to go over the full development slate for the network. When it came time to talk about reality programs, he jumped right in and asked about "Idol." Mr. Darnell was ready with his plans for how to execute the format. "Here's what I want to do," he began.
Mr. Murdoch cut him off. "You don't change a thing," he said, according to one of the Fox executives in the meeting. "This show works in England. And you're going to make the same show they made in England. The problem with you Hollywood people is you always want to change things and you ruin everything."
Mr. Murdoch had not likely studied the structure of the British format to determine that it was flawless. But he did know that the network would not have "Idol" had he not insisted on it.
No one would think of challenging Mr. Murdoch's views, but some Fox executives really did believe that the British format had some obvious flaws. For one thing, it had two hosts, which surely made the show seem unnecessarily cluttered. And the four-judge panel invited trouble because it was an even number. If the judges split two to two, the format called for Mr. Cowell to break the tie, but that seemed actually to reduce the number of judges to one.
FOX had not signed Mr. Cowell to a contract — at his insistence. He told the Fox executives, "I'll do one season and see how it goes." That was music to the ears of the Fox group, still worried about the expense of this little summer show that had suddenly grown to 15 episodes. Nobody really knew how the show would do. Mr. Cowell was still emphasizing that he was in it not for the fame or the salary, but for the money that would come from having yet another hot artist for his label. He did not even acquire an American agent — not right away.
The whole Fox network operation impressed Mr. Cowell because there was never a hint of an attempt to censor him or to turn him into a sweetheart of a guy. Fox seemed to him to be bravely acknowledging that the American audience, like the British audience, was ready to rebel against what Mr. Cowell called "the terrible political correctness that invaded America and England."
To Mr. Cowell, it looked as if Fox was going to allow the audience to see something that wasn't sanitized for a change. They would embrace the fact that with Mr. Cowell doing the talking, "lots of useless people were going to be told that they were useless."
The selection of the other judges went relatively smoothly. When Fox brought in Randy Jackson, the onetime bass player for the band Journey who became a successful producer and talent manager for Columbia Records, Mr. Cowell liked him immediately. When Mr. Cowell heard that Paula Abdul would also be named a judge, Mr. Cowell thought that she was also a solid choice, given her long music career in the United States.
Mr. Cowell did not meet Ms. Abdul until the first round of auditions for the show, which took place in Los Angeles. At that point, no one at Fox had ever even seen the three judges interact with one another. A fourth judge had still not been chosen, but given how much time the auditions were expected to take, the idea was to start with three and, if a fourth was found, to add him or her later.
Almost nothing was said among the judges before the first auditions rolled. Ms. Abdul seemed quiet and polite to Mr. Cowell; Mr. Jackson was affable. The first singers came in. They had already been screened, of course, and included a healthy mixture of respectable warblers and tone-deaf screechers.
This was teed up for Mr. Cowell, who unleashed his lash on every offending wannabe. He told one girl to get a lawyer and to sue her vocal coach. Others he labeled with such terms as wretched, horrid, pathetic. When one kid said he would someday regret all the hearts he was breaking, Mr. Cowell dismissed him with the line, "You're a loser."
The chorus of put-downs was clearly not what Ms. Abdul had been expecting. Several times during the first day, she looked over at Mr. Cowell in shock. He took notice. Apparently, Ms. Abdul had been anticipating the kind of audition that American kids usually got: "Oh, you were great! Thanks, we'll let you know." Instead, they were leaving either angry or in tears.
After the taping, Mr. Cowell cornered the producers. "I think Paula is going to walk," he told them. "I don't think she's going to want to continue to do the show." Ms. Abdul did not quit, but the relationship between her and Mr. Cowell was instantly tense. Their fractiousness on the air in those early shows was definitely not a put-on, Mr. Cowell said.
As the auditions moved on to a second round, Mr. Cowell remained concerned about how Ms. Abdul was going react to his give-no-quarter style. Just before the taping was to begin, one of the newer American producers came up to him with a long sheet of paper in his hand. He offered it to Mr. Cowell.
"What is it?" Mr. Cowell said.
"We've written a script for you today," the producer said.
"What do you mean a script?" the befuddled Mr. Cowell said.
"We've written put-downs for you, more put-downs," the producer said.
"What do you mean, you've written me put-downs?"
"Well, you're scripted, aren't you?" the producer said.
"No, I'm not scripted," Mr. Cowell said, now more appalled than surprised.
"Well, do you want these?" the producer said, offering the list again.
"No!" Mr. Cowell said, utterly indignant at the insult. Apparently these people were accustomed to everything being scripted.
AFTER the auditions, Mr. Cowell flew home to London. He was confident that the show would make great television. He had no idea if it would break through and be a hit, because he felt that he could not predict American tastes the way he could British tastes. But he was more than satisfied with how the auditions had gone. He would return for the live-performance shows just after the first few editions of "American Idol" went on the air.
Mr. Cowell was back at his day job in London on June 11, 2002. He had music artists and selling records on his mind, not "American Idol." The fact that the show had gone on the air the previous night in the United States had slipped his mind.
About 3 p.m. London time, he got a call. It was one of the "Idol" staff members in Los Angeles. When Mr. Cowell picked up the phone, the guy on the other end was so excited that he could hardly get the words out.
"Simon, this is amazing; it's a hit," the voice said.
Confused for a moment, Mr. Cowell said: "What are you talking about? What's a hit?"
" 'American Idol.' We opened last night, and the ratings are going through the roof."
"Fantastic!" Mr. Cowell said. "I'm really pleased."
The report was only a slight exaggeration. "Idol" was the most-watched show on American television, with 10 million viewers, on the Tuesday when it had its premiere; the next night it eclipsed 11 million. Both ranked even better among the young viewers whom Fox coveted, beating all competition in the 18-to-49 age group and, even better, finished first and second for the week among viewers 18 to 34.
Mr. Cowell immediately embarked on a round of publicity, doing 50 interviews with American radio stations in one day alone. Of course, the phenomenon that would soon dominate American pop culture — and ignite Fox on a spectacular ratings run toward real competitive balance with the other three networks — was only beginning. Within a matter of weeks, Fox was making arrangements to bring "Idol" back in the regular season, starting the following January.
"American Idol" would not be only the "game changer" that Mr. Grushow and Fox had been searching for.
It would be a business-changer for all of network television.
April 30, 2006
How a Hit Almost Failed Its Own Audition
By BILL CARTER
Network television programmers face a challenging job, though not a complicated one: they need to find hits. That's why they spend millions to find and hire talented writers, actors and producers. In many cases they would be wiser to invest in a catcher's mitt, because really big hits, ones that can transform the fates of networks — and of network executives — tend to fall from the sky. Here is the story of how "American Idol," the biggest hit on television, hovered over every network in 2001, waiting for one of them to grab it. This article is adapted from "Desperate Networks" by Bill Carter, a reporter for The New York Times. Doubleday will publish the book on Tuesday.
SIMON COWELL sat at a meeting in Los Angeles with executives from someplace he had never heard of, something called the UPN network. Mr. Cowell, a British music executive, had never pitched a television show in America before — and the way things were going, he felt as though he never would again.
The UPN executives who sat across the table from Mr. Cowell at that meeting in April 2001 clearly had no clue who this guy was, and, apparently, even less interest in finding out. Maybe they knew his business partner, Simon Fuller, from his leadership of the Spice Girls. Surely, they had heard of the Spice Girls. But, then again, as Mr. Cowell checked those blank, uninterested faces, maybe not.
No matter. Mr. Cowell had enormous faith in the idea that he and Mr. Fuller had for a music-based television show. Mr. Fuller was the most successful manager of music acts in Britain and he, Mr. Cowell, was the most successful artist and repertoire man — that is, music label talent manager — currently working there. They both knew how to launch new singing artists, and now they had an idea for a show that would allow them to utilize their talents on camera.
Despite the wall he sensed going up at the UPN meeting, Mr. Cowell, never cowed, simply plowed ahead with his pitch. "What this is really about is the American dream," Mr. Cowell told the American executives in his smooth British tones. He laid out the format for the show that he and Mr. Fuller were calling "Pop Idol" in Britain, describing how exciting this show would surely be. When Mr. Cowell wrapped up his comments, the room went quiet — stone silent.
At the opposite end of the table, a young woman executive, whom Mr. Cowell had identified in his head as the "lippy second-in-command," seemed to be calculating whether or not this truly was the end of the presentation.
"And what exactly do you think we're supposed to be doing for you?" the woman said, dismissively.
"Well, actually, sweetheart," Mr. Cowell replied, applying just a dash of acid, "it's more a question of what I could be doing for you."
Again a terrible silence fell. Then the woman piped up: "Well, we'll get back to you."
Mr. Cowell said he had heard that line before — too many times for it to bother him during his sojourn in the United States trying to spark some American interest in this hot idea. He and Mr. Fuller and a third partner, yet another Simon — Simon Jones, an executive with Thames Television — had paid calls to the broadcast networks, to MTV and to other cable networks. Every one of them had a free shot that April at landing the show that the three Simons were putting on offer. No one showed the least interest, and many of the network executives offered shoulders so cold that Mr. Cowell could have chilled his wine on them. Uniformly, they had been, Mr. Cowell was convinced, the worst, most appalling meetings of his life.
The contrast with how "Pop Idol" had been sold in Britain could not have been sharper. Mr. Cowell and Mr. Fuller met with representatives of the British network ITV, spent what Mr. Cowell estimated was no more than 30 seconds describing the idea, and they had a deal. But, of course, the two Simons had enormous reputations in the British entertainment world, and they were entering a market that had already embraced music-oriented reality shows.
In Britain, "Pop Stars," a show that was originally developed in Australia and traced the formation of a singing group, had engrossed the nation. Another music show, "Fame Academy," had also done extremely well.
Mr. Cowell had been invited to be a judge on the first edition of "Pop Stars," and, at first, had accepted. But he quickly had misgivings about being a person who ran a music label going on television to demonstrate how to put together a group. Mr. Cowell thought it was "like a magician showing how you saw somebody in half." He bowed out.
When Mr. Cowell got a first glimpse of "Pop Stars," however, he knew he had made a mistake. The show looked like a piping hot hit to him — though he had an instant insight. To him, the attractive part of "Pop Stars" was the round of auditions to select the band members. He thought that, as constituted, "Pop Stars" had no ending. With Mr. Fuller he conceived a show built around seasonlong tryouts with the winner announced at the end.
What Mr. Cowell told ITV was this: "It will have all the fun of 'Pop Stars,' but we can do it better. We can do it a lot harsher than on 'Pop Stars,' and the public will vote and choose the winner. And we won't be relying on the music to make the show successful: it will be a soap opera."
Mr. Cowell also volunteered himself as a judge, knowing that he had the precise expertise called for in selecting a singing star. Mr. Fuller and his company, 19 Entertainment, owned the show along with Fremantle Media, a big European production company. Mr. Cowell took no ownership stake, but he did get royalty rights for his label, Syco Records, a part of the BMG Music Group, on every recording released by an "Idol" performer worldwide. That was the essence of the show's appeal for Mr. Cowell.
All he was concerned with was that the right person would win, so that he would get access to a good artist. If the show was a hit, so much the better; Mr. Cowell's new artist was more likely to sell a lot of records that way.
When Mr. Cowell started shooting "Pop Idol" in England in the summer of 2001, the production plan called for four judges to sit in an audition room while contestants trooped in, one by one. The judges would discuss each singer after he or she left the room. Nothing more specific was spelled out.
The first auditions took place in Manchester. But by the time five or six singers had walked through, sung and then had their performances rehashed by the judges after they had left the room, Mr. Cowell was almost crawling up the walls.
"I'm dying in here," he told the producers. "This is not like a real-life audition." He turned to one of the other judges, the veteran British pop producer Pete Waterman, and said: "We have to actually tell the performers to their faces what we thought. We've just got to tell these boys and girls the truth. They're rubbish."
Mr. Cowell had invited Mr. Waterman to work as a judge, expecting him to be what Mr. Cowell described as the "nasty" one. But Mr. Waterman got more emotional on the show than Mr. Cowell expected. (It was published in the British press that he actually teared up at one performance). Mr. Cowell, meanwhile, acted no differently on the air than he did at real auditions — he was cold and distant. And his comments reflected that.
As the show took off after its premiere that October, the British press concentrated on Mr. Cowell and his barbed comments. He was the nasty one, the "mouthy" one. The show quickly began to revolve around Mr. Cowell and his withering appraisals of the wretched talent being brought before him.
"Pop Idol" was the hit of the year in Britain. The two finalists both released albums after the show concluded and sold millions of copies. Mr. Fuller had two new hit artists to manage; Mr. Cowell's label had two huge-selling albums. Their collaboration was a ringing success — and they were just getting started.
Alix Hartley, a British-born talent agent with an expertise in music, who worked for the Creative Artists Agency, the heavyweight Hollywood talent agency, was a natural to represent Mr. Fuller in the challenge of going back to the networks in the fall of 2001 and finding "Pop Idol" a home on American television.
Given how both "Who Wants to Be a Millionaire" and "Survivor" — both conceived by British producers — had emerged as hits on American television in the summer months, C.A.A.'s strategy was to pitch "Pop Idol" around as a perfect new reality programming vehicle for the summer of 2002. It was light, entertaining and not very expensive to produce. As an added advantage, having started a 15-week British run in October, it would have fully executed weekly editions on tape to serve as the template for the American version.
ANDREA WONG, who ran the reality-programming department for ABC, was an ideal target for the C.A.A. pitch. She was aggressively seeking reality programs and had been closely watching the British market in the wake of her network's failure to secure "Survivor" when it had twice been in ABC's clutches.
But C.A.A. and the producers of "Pop Idol" ran into a problem that "Survivor" never had to face. Music had already failed in the United States in reality formats on two networks, one being ABC.
That network tried a show in 2000 called "Making the Band," about assembling a boy-band singing group. Though it had a small following, mostly among pubescent girls, the show simply could not cross over into a wider audience. The music format was blamed. Music had become just too stratified, the argument went, to ever build a wide-enough appeal in the United States to succeed on the scale that an American network television show required.
The WB network, which was mainly the network of pubescent girls, tried a similar format the next season with a show that the network called "Pop Stars," a format derived from the Australian and British models of the same name — only with an-all girl group. It, too, found only a niche audience.
Ms. Wong knew all of that when C.A.A. came in touting "Pop Idol." She passed. C.A.A. next met with NBC's reality executives. They passed. The agency never set up a formal meeting with CBS's reality division, feeling as though an initial phone call to CBS had fallen utterly flat.
That left Fox. The British producers had gotten nowhere in the spring when they tried to interest Fox's reality division, headed by Mike Darnell, in "Pop Idol." But C.A.A. made a new effort anyway. This time Ms. Hartley of C.A.A. and Mr. Fuller — without Mr. Cowell this time — went in to see Mr. Darnell himself.
Mr. Fuller pitched his idea with fervent passion, and that impressed Mr. Darnell. He really liked the notion that the format would essentially be all audition, complete with a lot of really woeful early performances. Mr. Darnell had never liked the band-making shows once they got past the auditions. Here was a format in which the auditions, replete with people making cringe-inducing fools of themselves, would rule.
Mr. Darnell, thinking of summer budgets at Fox, wanted to know if the show had sponsorship attached. Ms. Hartley told him that C.A.A. was working on that very angle. Mr. Darnell told Ms. Hartley and Mr. Fuller that they should bring up the idea with Sandy Grushow, the head of entertainment for Fox, and his chief lieutenant, Gail Berman.
When Mr. Grushow and Ms. Berman heard the pitch, both had the same reaction: tepid. A talent contest did not sound like inspiring television in the 21st century — or like a breakout hit, for which Fox had an increasingly searing need at that point.
But both executives knew that the network could also use something that might pass for fresh summer programming. The problem was, Fox was out of money. The program budget for the year was exhausted, bone dry.
Mr. Grushow told the C.A.A. representatives that Fox was simply not going to pay a license fee for this program — if it was going to get on the air, it would have to be as a fully sponsored broadcast. "We don't know much about this show," Mr. Grushow told them. "But if we can get it for nothing, it's sort of a no-brainer."
C.A.A. indicated that, of course, it could line up sponsors. Fox said: Come back to us when you do.
By this point, early in winter, "Pop Idol" had become the talk of Britain. Fox had made no effort to secure the show, so C.A.A. went back to Ms. Wong from ABC, armed with those mighty ratings from the British run. She asked to see a tape of the British show. That was encouraging. A tape was delivered. Ms. Wong watched it — and passed again.
The impasse with Fox continued. C.A.A. heard nothing from Mr. Darnell. Ms. Berman and Mr. Grushow continued to press for a fully sponsored show; nothing was happening, despite the fabulous success in Britain.
But even as talks with Fox dragged on, C.A.A. was trying to exploit a connection that some at the agency believed might play out to their advantage. Back in October, several C.A.A. executives had met with Elisabeth Murdoch, daughter of Rupert Murdoch, the founder and chief executive of the News Corporation, which owns Fox. The meeting took place at Mipcom, the international television programming festival in Cannes, France. A blossoming relationship took hold there.
With the talks about "Idol" stalled in Los Angeles, the C.A.A. representatives at one point mentioned the show in a conversation with Ms. Murdoch, who ran the News Corporation's most important television operation in England, the BSkyB satellite channel. She, of course, was witnessing the phenomenon of "Pop Idol" firsthand, on her home TV set.
Fortunately for C.A.A., Ms. Murdoch flat-out loved the show. Hearing that her father's American network had yet to act on making a deal for the United States rights, she decided to give the process a helpful nudge. She called her father and told him how much she loved "Pop Idol" and how big the show was becoming in England. She urged him to buy the rights for Fox.
Mr. Murdoch put in a call the next day to Peter Chernin, his No. 2 at the News Corporation and the top decision-maker on all the biggest moves made by the Fox network. "What's going on with this show 'Pop Idol,' Peter?" Mr. Murdoch asked Mr. Chernin. "It's a big hit in England. I spoke to Liz and she says it's great."
Mr. Chernin was familiar enough with the situation to report that Fox's network people had been talking about it with the agency, discussing potential advertising backers. "We're still looking at it," he said.
Mr. Murdoch shot back: "Don't look at it. Buy it! Right now."
With those marching orders ringing in his ears, Mr. Chernin followed up quickly, calling Mr. Grushow and Ms. Berman. He asked them the status of "Pop Idol." They told him that they were still waiting for the advertiser sponsorships to come through.
"Just close the deal," Mr. Chernin said. He explained the call from Mr. Murdoch.
Mr. Grushow said, "We'll get it closed today."
The actual order for the series suddenly changed as well. Instead of an eight-episode summer order, Fox began asking C.A.A. for the rights to broadcast 15 episodes — the same duration as the show in Britain. The C.A.A. agents concluded that one of the Murdochs, or maybe both, had insisted that the show be done exactly as it was in England.
That did not mean that Fox would import the British hosts and judges. Fox fully expected to hire figures from the American music industry for those jobs. But after the deal was concluded, and Mr. Grushow finally was able to watch a tape of the British version, he told Ms. Berman that he was taken by the nastily charismatic figure on the British judging panel. "I think as part of the deal, we should insist on bringing this guy over as a judge," he said. At that point, he could not remember Simon Cowell's name.
"Pop Idol" made Mr. Cowell one of the most talked-about cultural figures in Britain in the winter of 2002. He was a tabloid newspaper's dream: seen by millions every week on television, saying something outrageously quotable ("You're a disaster"), doing something unconscionably cruel (several young women left the auditions convulsed in tears after hearing his corrosive assessments of their talents) and tirelessly promoting his program (by doing every sort of interview in print and on television and radio).
Mr. Cowell said he was pleased when he heard that the show had finally sold in the United States but mildly shocked when he learned that Fox was requesting that he come along to be a judge on the American version. He had not planned on turning himself into an international television star; he said he wanted only to make the show a hit for the benefit of his record label.
At first he had doubts about whether he knew enough about American music to judge American singers. He was also concerned because of the way American television executives functioned during those hideous meetings in the spring. He expected that some genius at the American network was bound to try to water down the show, and especially his honestly acerbic comments. He would have no interest in a sweetened version of "Pop Idol."
Then Kevin Warwick, one of the producers of the British show, called. "Look, Simon, we're going over to produce the show in America," he said. "I will look after your back again. You won't have to compromise what you do. You can be yourself."
Mr. Cowell asked, "So I can really be the same as I was in England?"
Mr. Warwick assured him that he could.
A few weeks later, Mr. Cowell arrived in Los Angeles for his first round of meetings with Fox and the American producer, Brian Gadinsky. At first they considered rechristening it "America's Idol." Mr. Darnell thought that made it sound as if it might be about a New York fireman, so he suggested "American Idol." (Nobody wanted "pop" in the title because nobody in the music business in the United States ever used the word "pop" anymore — with the exception of Michael Jackson — and because "Pop Stars" had been a failure for the WB network.)
Mr. Murdoch, as he often did, sat in on a meeting that winter to go over the full development slate for the network. When it came time to talk about reality programs, he jumped right in and asked about "Idol." Mr. Darnell was ready with his plans for how to execute the format. "Here's what I want to do," he began.
Mr. Murdoch cut him off. "You don't change a thing," he said, according to one of the Fox executives in the meeting. "This show works in England. And you're going to make the same show they made in England. The problem with you Hollywood people is you always want to change things and you ruin everything."
Mr. Murdoch had not likely studied the structure of the British format to determine that it was flawless. But he did know that the network would not have "Idol" had he not insisted on it.
No one would think of challenging Mr. Murdoch's views, but some Fox executives really did believe that the British format had some obvious flaws. For one thing, it had two hosts, which surely made the show seem unnecessarily cluttered. And the four-judge panel invited trouble because it was an even number. If the judges split two to two, the format called for Mr. Cowell to break the tie, but that seemed actually to reduce the number of judges to one.
FOX had not signed Mr. Cowell to a contract — at his insistence. He told the Fox executives, "I'll do one season and see how it goes." That was music to the ears of the Fox group, still worried about the expense of this little summer show that had suddenly grown to 15 episodes. Nobody really knew how the show would do. Mr. Cowell was still emphasizing that he was in it not for the fame or the salary, but for the money that would come from having yet another hot artist for his label. He did not even acquire an American agent — not right away.
The whole Fox network operation impressed Mr. Cowell because there was never a hint of an attempt to censor him or to turn him into a sweetheart of a guy. Fox seemed to him to be bravely acknowledging that the American audience, like the British audience, was ready to rebel against what Mr. Cowell called "the terrible political correctness that invaded America and England."
To Mr. Cowell, it looked as if Fox was going to allow the audience to see something that wasn't sanitized for a change. They would embrace the fact that with Mr. Cowell doing the talking, "lots of useless people were going to be told that they were useless."
The selection of the other judges went relatively smoothly. When Fox brought in Randy Jackson, the onetime bass player for the band Journey who became a successful producer and talent manager for Columbia Records, Mr. Cowell liked him immediately. When Mr. Cowell heard that Paula Abdul would also be named a judge, Mr. Cowell thought that she was also a solid choice, given her long music career in the United States.
Mr. Cowell did not meet Ms. Abdul until the first round of auditions for the show, which took place in Los Angeles. At that point, no one at Fox had ever even seen the three judges interact with one another. A fourth judge had still not been chosen, but given how much time the auditions were expected to take, the idea was to start with three and, if a fourth was found, to add him or her later.
Almost nothing was said among the judges before the first auditions rolled. Ms. Abdul seemed quiet and polite to Mr. Cowell; Mr. Jackson was affable. The first singers came in. They had already been screened, of course, and included a healthy mixture of respectable warblers and tone-deaf screechers.
This was teed up for Mr. Cowell, who unleashed his lash on every offending wannabe. He told one girl to get a lawyer and to sue her vocal coach. Others he labeled with such terms as wretched, horrid, pathetic. When one kid said he would someday regret all the hearts he was breaking, Mr. Cowell dismissed him with the line, "You're a loser."
The chorus of put-downs was clearly not what Ms. Abdul had been expecting. Several times during the first day, she looked over at Mr. Cowell in shock. He took notice. Apparently, Ms. Abdul had been anticipating the kind of audition that American kids usually got: "Oh, you were great! Thanks, we'll let you know." Instead, they were leaving either angry or in tears.
After the taping, Mr. Cowell cornered the producers. "I think Paula is going to walk," he told them. "I don't think she's going to want to continue to do the show." Ms. Abdul did not quit, but the relationship between her and Mr. Cowell was instantly tense. Their fractiousness on the air in those early shows was definitely not a put-on, Mr. Cowell said.
As the auditions moved on to a second round, Mr. Cowell remained concerned about how Ms. Abdul was going react to his give-no-quarter style. Just before the taping was to begin, one of the newer American producers came up to him with a long sheet of paper in his hand. He offered it to Mr. Cowell.
"What is it?" Mr. Cowell said.
"We've written a script for you today," the producer said.
"What do you mean a script?" the befuddled Mr. Cowell said.
"We've written put-downs for you, more put-downs," the producer said.
"What do you mean, you've written me put-downs?"
"Well, you're scripted, aren't you?" the producer said.
"No, I'm not scripted," Mr. Cowell said, now more appalled than surprised.
"Well, do you want these?" the producer said, offering the list again.
"No!" Mr. Cowell said, utterly indignant at the insult. Apparently these people were accustomed to everything being scripted.
AFTER the auditions, Mr. Cowell flew home to London. He was confident that the show would make great television. He had no idea if it would break through and be a hit, because he felt that he could not predict American tastes the way he could British tastes. But he was more than satisfied with how the auditions had gone. He would return for the live-performance shows just after the first few editions of "American Idol" went on the air.
Mr. Cowell was back at his day job in London on June 11, 2002. He had music artists and selling records on his mind, not "American Idol." The fact that the show had gone on the air the previous night in the United States had slipped his mind.
About 3 p.m. London time, he got a call. It was one of the "Idol" staff members in Los Angeles. When Mr. Cowell picked up the phone, the guy on the other end was so excited that he could hardly get the words out.
"Simon, this is amazing; it's a hit," the voice said.
Confused for a moment, Mr. Cowell said: "What are you talking about? What's a hit?"
" 'American Idol.' We opened last night, and the ratings are going through the roof."
"Fantastic!" Mr. Cowell said. "I'm really pleased."
The report was only a slight exaggeration. "Idol" was the most-watched show on American television, with 10 million viewers, on the Tuesday when it had its premiere; the next night it eclipsed 11 million. Both ranked even better among the young viewers whom Fox coveted, beating all competition in the 18-to-49 age group and, even better, finished first and second for the week among viewers 18 to 34.
Mr. Cowell immediately embarked on a round of publicity, doing 50 interviews with American radio stations in one day alone. Of course, the phenomenon that would soon dominate American pop culture — and ignite Fox on a spectacular ratings run toward real competitive balance with the other three networks — was only beginning. Within a matter of weeks, Fox was making arrangements to bring "Idol" back in the regular season, starting the following January.
"American Idol" would not be only the "game changer" that Mr. Grushow and Fox had been searching for.
It would be a business-changer for all of network television.
Subscribe to:
Comments (Atom)